


Subsidising healthcare for children in Mali substantially increased necessary care-seeking while generating only minimal unnecessary use.
It is sometimes striking how policy conversations about the same issue play out completely differently in high-income and low-income countries. Take the debate around the role of payments at the point of care for healthcare demand.
For low-income settings, the policy trade-off is typically framed around access barriers versus budget burdens. The Bamako initiative in 1987 by many African countries stipulated partial cost recovery for health system sustainability through the sale of essential drugs (Garner 1989). But in the last 20 years, the global health community has shifted focus on achieving universal health coverage (UHC) and removing user fees in order to combat the continued high mortality rates of mothers and children (Robert and Ridde 2013). In this context, high demand for free or low-cost health services is mostly treated as a problem of inadequate financing and shrinking aid budgets (Financing Alliance for Health 2025).
Contrast this with the debate around co-pay in the research on US health insurance. Here, a common framing is that any increase in healthcare demand in response to a lower out-of-pocket price is evidence of “ex post moral hazard” (Einav and Finkelstein 2018). This goes back to Pauly (1968)’s comment on an overlooked “commitment problem”: patients who are willing to pay, say, X per year to maintain their health and would be willing to buy insurance up to X, may still consume much more healthcare than X once they are covered by insurance. In other words, patients with no co-pay are overconsuming healthcare services relative to what these services are worth to them.
The risk of overuse obviously translates to subsidised healthcare. If it is free, a patient may see a doctor even when it is not really necessary. This risk does not get a lot of attention in global health. At the same time, treating any increase in healthcare utilisation as problematic is of course simplistic. It assumes that the amount X patients can pay for healthcare without subsidies is at an optimal level. Yet in the context of children dying preventable deaths, the whole point of lowering user fees is to make it easier for vulnerable populations to see a doctor. In fact, research on health insurance in LMICs often reports the lack of overall utilisation effects as a somewhat disappointing or even puzzling result.[1]
Assessing the value of healthcare
So where does this leave us? What share of healthcare demand induced by a subsidy is meeting an unfilled need and reducing underuse, how much is overuse?
To be able to answer this question, we need to understand whether individual instances of care-seeking are high value or not. For low-income households, observed demand at full prices is unlikely to reflect the full value of healthcare. Financial constraints may prevent them from saving enough to cover unexpected healthcare expenses. Caretakers may not internalise the true value of care, for example, because they do not understand the risks of delaying care for a seriously ill child. At the same time, households may still overuse healthcare when prices are zero or very low.
These frictions imply that we need to measure the value of care in other ways, and this is difficult for several reasons. Unlike preventive care such as vaccines or malaria bed nets, whether and when a person needs acute healthcare depends on their current illness status. In addition, even if a sick child ex ante should be seen by a doctor based on risks, the illness may still pass, even without treatment. Better access to care maps only indirectly into better (long-term) health outcomes.
A novel approach to measuring need for care for children
In Sautmann, Brown, and Dean (2025), we took a different approach: we collected detailed symptom calendars over nine weeks for all 1,768 children in our sample and applied guidelines derived from WHO triage algorithms for low-resource settings, the Community Integrated Management of Childhood Illnesses (C-IMCI) (Rosales and Weinhauer 2003), to determine whether a child should be seen by a (formal) healthcare provider. We did this as part of a randomised controlled trial in which half of our sample received a subsidy programme that provided free medical care for the most common childhood illnesses at the local clinic, amounting to a nearly 70% reduction in out-of-pocket cost.[2] This design allowed us to test how a subsidy programme affects care-seeking conditional on ‘need for care’ according to the C-IMCI, or in other words, whether a given doctor visit was necessary or unnecessary.
Our data gave us many insights into the (health) lives of children in Bamako. They live in traditional families with on average 6.2 members, often sharing a compound with other households. Not unlike in a typical US day care, they are constantly sniffling. On average, children had cold symptoms on nearly 20% of all recorded days. But they also have much more serious illnesses; for instance, fever, severe vomiting, and difficulty breathing occur on 9%, 1.3%, and 1.7% of days, respectively. In the control group, about half of all illness spells eventually need care according to the C-IMCI, but in only 11% of them does the child actually see a doctor.
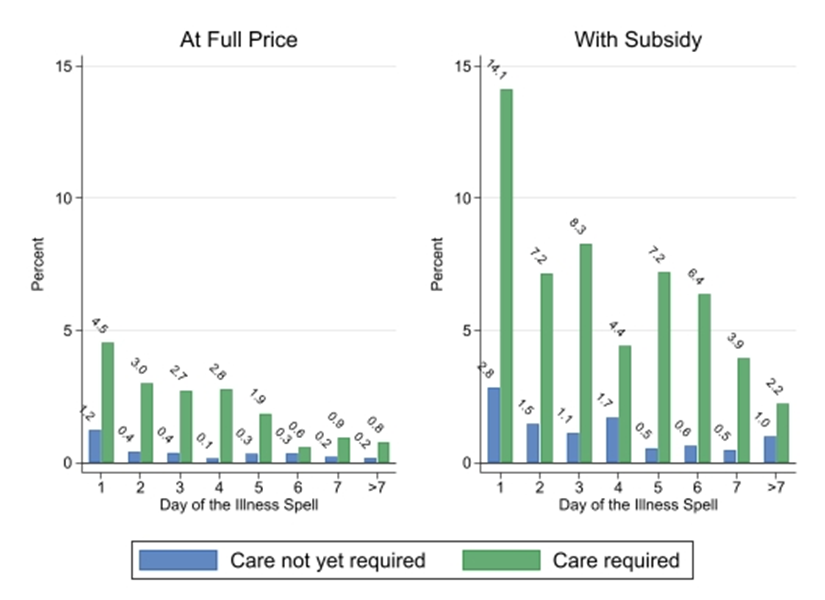
The subsidy changed care-seeking drastically. Figure 1 below shows the probability of a doctor visit on every day of an illness spell, conditional on need for care. In the control group, care was sought on less than 4.5% of the days it was required, and when not required, it was negligible (0.1–1.2%). With the subsidy, care-seeking was nearly three times more likely, with up to 14.1% probability when it was needed, and between 0.5% to 2.8% probability when it was not required; in other words, the subsidy induced much more needed than unnecessary care.
Figure 1: Daily probability of care-seeking by early vs. care-required classification
Our data illustrates several other insights. First, even with a generous subsidy and despite the strong effects on demand for (necessary) care, these children still receive nowhere near a minimum standard of care. Out of all spells that ever entered ‘care required’ status, only about 29% received medical attention, and often several days late, exposing the child to risks and discomfort.
Second, even if day-by-day care-seeking was very low, cumulatively it is still the case that a doctor visit occurred in 8.8–10.9% of spells that never required care. A government official tracking wasteful health spending at public clinics would find that about 25% of all clinic visits were unnecessary. But our home observation adds nuance: out of all illness spells, those that ended in a doctor visit despite not needing care make up less than 5%, whereas those that needed a doctor visit but did not get it made up 38%. In other words, the more prevalent problem from the perspective of children’s wellbeing remains underuse, not overuse.
Policy implications for global health
Illness spell data collected in the home makes visible the many instances of serious illness in children that never receive any formal care.
Our results strongly suggest that the cost of care is a primary barrier to effective care-seeking in the urban population we study, even at public clinics where healthcare is more affordable than in the private sector.
At the same time, families are almost six times more likely to visit a doctor when symptoms warrant it according to the C-IMCI than otherwise. This suggests that, for example, health education policies teaching parents the signs of serious illness may not be particularly effective, and without going into detail, this is indeed what our study arms suggest that test the effects of community health worker visits on care-seeking.
Further progress on improving access to healthcare for children should prioritise the removal of user fees, along with potentially other barriers to access, such as non-monetary costs. Even at highly subsidised prices, the healthcare needs of children in low income households are likely only incompletely met.
References
Einav, L, and A Finkelstein (2018), “Moral hazard in health insurance: What we know and how we know it,” Journal of the European Economic Association, 16: 957–982.
Financing Alliance for Health (2025), “Abolishing user fees: A gender imperative in a changing aid landscape,” Unpublished manuscript.
Garner, P (1989), “The Bamako initiative,” British Medical Journal, 299: 277–278.
Pauly, M V (1968), “The economics of moral hazard: Comment,” American Economic Review, 58: 531–537.
Robert, E, and V Ridde (2013), “Global health actors no longer in favor of user fees: A documentary study,” Globalization and Health, 9: 29.
Rosales, A, and K Weinhauer (2003), "C-IMCI: Community Integrated Management of Childhood Illness," Catholic Relief Services.
Sautmann, A, S Brown, and M Dean (2025), “Subsidies, information, and the timing of children’s health care in Mali,” Review of Economics and Statistics: 1–32.