





A group therapy programme only reduced depression rates among adolescent girls in Uganda in the short-term. Adding a cash transfer to the programme backfired, likely due to the COVID-19 pandemic and associated stressors.
Mental health disorders are a major burden for adolescent girls worldwide
Depression and anxiety related disorders are among the leading contributors to years lived with a disability for adolescents worldwide, and young women are especially at risk (Guthold et al. 2021). Mental health disorders developed during adolescence do not just affect current wellbeing; they can also affect the trajectory of a young person’s life, influencing human capital accumulation via increased risky decision-making, lower educational achievement, and lower self-efficacy and self-esteem (Patel et al. 2007). Despite the critical need, mental health disorders are often left untreated, especially in low- and middle-income countries, due in part to the high cost of mental healthcare and shortage of well-trained specialist providers (Chisholm et al. 2016).
Addressing this gap requires identifying easily scalable and cost-effective solutions. One class of interventions that has received considerable attention is manualised talk therapy–i.e. cognitive behavioural therapy or interpersonal therapy–motivated, in part, because it can be adapted to be delivered in groups and by trained non-specialist providers. A small but growing evidence base has found that such interventions can result in sizable improvements in mental health, but evidence of sustained impacts remains scarce; that is, beyond the 3- to 12-month post-intervention periods evaluated in most studies (Singla et al. 2017). Furthermore, little is known about potential knock-on effects on human capital accumulation and cognition, which would indicate potentially transformative impacts.
Evaluating a low-cost, scalable approach for treating adolescent mental health
Our research seeks to provide a proof-of-concept for an easily scalable model for delivering therapy to adolescents (Baird et al. 2025). We partnered with StrongMinds Uganda (SMU), which specialises in training non-specialist providers to deliver group-based interpersonal therapy (IPT-G), and BRAC Uganda, which operates the ‘Empowerment and Livelihood for Adolescents’ (ELA) clubs. The ELA clubs provide a safe space for adolescent girls to socialise and participate in life skills and vocational training programmes (Bandiera et al. 2017). The clubs are led by female mentors, typically aged 19 to 22, who are selected from the community, undergo low-intensity training, and receive a small stipend. SMU provided extensive training and supervision to the club mentors to deliver group interpersonal therapy to club attendees. The complementarities between BRAC’s adolescent empowerment programming and SMU’s group-based therapy programme made ELA clubs a promising avenue for improving adolescent mental health in a cost-effective and potentially scalable manner.
To evaluate the impact of this model, we designed a cluster-randomised trial in which 106 ELA clubs in and around Kampala were randomised into: (i) a control group, (ii) a therapy-only group (IPT-G), in which adolescents received 14 weeks of IPT-G led by the trained ELA club mentors and supervised by SMU staff, and (iii) a therapy+cash group (IPT-G+), in which adolescents were offered the same therapy followed by a one-time lump-sum unconditional cash transfer, announced and delivered after the end of therapy. The study participants, aged 13 to 19 and exhibiting symptoms of moderate to severe depression at baseline, were recruited from within the clubs’ catchment areas.
The challenge of rolling out a mental health programme during the onset of the COVID-19 pandemic
The IPT-G intervention took place in the second half of 2019, with cash transfers distributed immediately after the intervention and up until March 2020, just before the COVID-19 pandemic was declared. The first lockdown in Uganda began on March 18, 2020, and lasted until May 5, 2020, ushering in the start of a difficult period in Uganda, marked by political unrest and the world’s longest school closures (Figure 1).
Figure 1: Study timeline and major events in Uganda
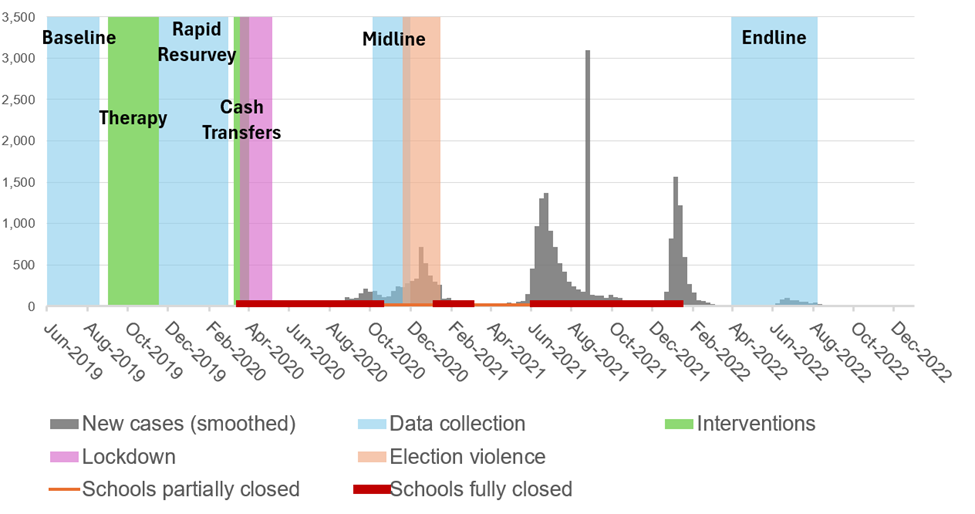
Sources: Case data obtained from Our World in Data COVID-19 case trackers (Mathieu et al. 2020); school closures data from UNESCO (2022); reporting on election violence by Human Rights Watch (2021); reporting on the lockdown by Reuters (2022).
Group interpersonal therapy helped reduce rates of depression up to one year later, but impacts dissipated two and a half years later
Eligibility for the study meant that all study participants were initially at risk of moderate to severe depression, measured by a Patient Health Questionnaire-8 (PHQ-8) score of 10 or above. By the 12-month follow-up, 18% of individuals in the control group had recovered and showed no symptoms of even mild depression (PHQ-8≤4), and 28% showed no signs of psychological distress as per the Generalized Health Questionnaire-12 (GHQ-12<3). These rates of recovery from depression and psychological distress were each 5 percentage points higher in the IPT-G group compared to the control group (Figure 2). Given the relatively small but statistically significant impacts on mental health, we also find limited impacts on human capital accumulation, with modest positive impacts on school enrolment, delayed marriage, desired fertility, and time preferences. Both the mental health and human capital effects had almost entirely dissipated by the two-and-a-half-year follow-up.
Figure 2: Impact estimates on primary mental health outcomes
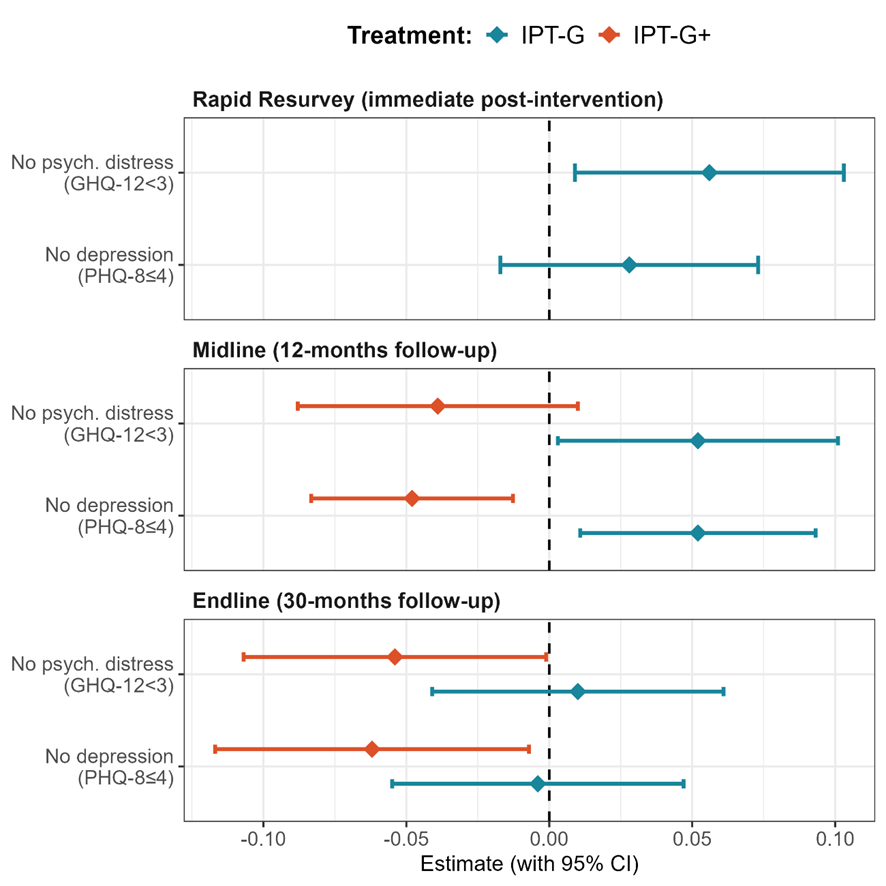
Note: This table shows ITT estimates of the impact of IPT-G and IPT-G+ on the primary mental health outcomes–the share of adolescents with a PHQ-8 score ≤4 and the share with a GHQ-12 score <3; The treatment indicators are combined in the Rapid Resurvey as the cash transfers were announced and delivered after the survey; All regression models include randomisation block fixed effects centred and fully interacted with all treatment indicators; Standard errors clustered at the club level; p-values are a t-test of the treatment effects coefficient = 0 and the corresponding q-values adjust for the false discovery rate as per Benjamini and Hochberg (1995).
Adding a cash transfer to the group therapy seems to have backfired, likely due to the destabilising impact of the COVID-19 pandemic
We hypothesised that the marginal impacts of the cash transfer, over and above therapy, would be positive on both mental health and human capital outcomes. The idea is that by easing day-to-day budget concerns and offering some insurance against negative shocks, cash transfers can create the mental space necessary to absorb the lessons and apply the behavioural skills learned in therapy. Much to our surprise, we instead found that offering cash with therapy led to an increase in depression and psychological distress relative to the therapy only group, which persisted until endline but was not reflected in any of the human capital outcomes.
The negative impact of cash is likely due to the COVID-19 pandemic. The pandemic caused significant hardship, with nearly 50% of adolescents reporting at the 12-month follow-up that their households had lost most or all of their income during the initial phase of the pandemic. While cash transfers may have initially raised aspirations among adolescent beneficiaries, they also became a source of frustration when families began relying on them to cover necessities. We find evidence that cash transfers increased tensions within the household (adolescents in the therapy+cash arm were more likely to report getting angry quickly and arguing more often than those in the therapy-only arm), potentially unravelling some of the positive impacts of therapy.
Implications for mental health programmes for adolescents
Our findings contribute to the growing evidence base on the potential of group-based therapy for treating mental health issues in low-resource settings, even though we find no evidence of long-term impacts. Unfortunately, we can only speculate whether the effects of therapy would have been larger or smaller had the pandemic not occurred, but it seems unlikely that therapy alone would have been transformative. The addition of a cash transfer to the therapy intervention raises important questions about the role of financial interventions in adolescent mental health programmes. Our findings underscore the need for a more nuanced approach to integrating financial support to promote adolescent welfare, taking into account adolescents’ potentially limited autonomy, intra-household power dynamics, and the broader socioeconomic context.
Overall, we highlight the challenge of tackling mental health among adolescents in low- and middle-income countries. Although there is ample evidence that adolescent programming–both mental health specific and otherwise–can improve mental health in the short term, effect sizes are often small and not sustained over time, even when they are large.
Still, lessons from our research, combined with broader internal monitoring and evaluation, led SMU to significantly revise its approach to delivering therapy for adolescents. Notably, this included developing separate models for in-school and out-of-school adolescents. SMU also decided to train teachers, rather than near-peer mentors, to lead IPT-G sessions, providing them with more intensive training. Further research is needed to evaluate the impact and cost-effectiveness of this revised approach.
References
Baird, S, B Özler, C Dell’Aira, L Parisotto, and D Us-Salam (2025), “Therapy, mental health, and human capital accumulation among adolescent girls in Uganda”, Journal of Development Economics, 176: 103473.
Benjamini, Y and Y Hochberg (1995), “Controlling the false discovery rate: A practical and powerful approach to multiple testing”, Journal of the Royal Statistical Society: Series B (Methodological), 57(1): 289–300.
Chisholm, D, K Sweeny, P Sheehan, B Rasmussen, F Smit, P Cuijpers, and S Saxena (2016), “Scaling-up treatment of depression and anxiety: A global return on investment analysis”, The Lancet Psychiatry, 3(5): 415–424.
Goldberg, D and P Williams (1988), "General Health Questionnaire".
Guthold, R, E W Johansson, C D Mathers, and D A Ross (2021), “Global and regional levels and trends of child and adolescent morbidity from 2000 to 2016: An analysis of years lost due to disability (YLDs)”, BMJ Global Health, 6(3): e004996.
Human Rights Watch (2021), "Uganda: Elections Marred by Violence".
Kroenke, K, T W Strine, R L Spitzer, J B Williams, J T Berry, and A H Mokdad (2009), “The PHQ-8 as a measure of current depression in the general population”, Journal of Affective Disorders, 114(1–3): 163–173.
Mathieu, E, H Ritchie, L Rodés-Guirao, C Appel, C Giattino, J Hasell, B Macdonald, S Dattani, D Beltekian, and E Ortiz-Ospina (2020), “Coronavirus pandemic (COVID-19)”, Our World in Data.
Patel, V, A J Flisher, S Hetrick, and P McGorry (2007), “Mental health of young people: A global public-health challenge”, The Lancet, 369(9569): 1302–1313.
Reuters (2022), "COVID-19 Tracker: Uganda".
Singla, D R, B A Kohrt, L K Murray, A Anand, B F Chorpita, and V Patel (2017), “Psychological treatments for the world: Lessons from low- and middle-income countries”, Annual Review of Clinical Psychology, 13(1): 149–181.
UNESCO (2022), “Education: From disruption to recovery”.