


Do we fully understand the impacts of emergency aid? New evidence from the 1984 Ethiopian famine suggests that emergency aid mitigates the impacts of large-scale disasters even decades later.
The number of natural disasters has dramatically increased since 1960 (EM-DAT and CRED/UCLouvain 2024). In 2024, 393 natural disasters occurred worldwide, affecting 167.2 million people and causing US$241.95 billion in economic losses (CRED 2025). Apart from the immediate impacts of these disasters (e.g. increasing mortality rate), they also have long-lasting detrimental impacts on health outcomes (Cunha and Heckman 2007, Maccini and Yang 2009, Dinkelman 2017). Without any mitigating strategies, the victims of such disasters in early life could experience severe health deterioration in adulthood.
A common ex-post coping strategy for disasters is emergency aid (also known as relief aid or humanitarian aid). The question is whether emergency aid can mitigate the negative impacts of disasters in the long run. Emergency aid is a short-term operation intended to provide vulnerable people with prompt assistance in response to a large-scale disaster (Fink and Redaelli 2011). It is therefore different from development aid that is designed as a mid- or long-term intervention to reduce poverty and chronic malnutrition, and to facilitate economic and institutional development. Whether the short-term oriented assistance of emergency aid can have long-term mitigating impacts remains an open and important question.
The 1984 Ethiopian famine and 1985 relief aid operation
To find an answer to this question, we study the Ethiopian relief operation in response to a large-scale devastating, drought-driven famine in 1984 (Di Falco and Han 2025). In 1984, Ethiopia was hit by an extremely widespread and intense drought, causing the great famine. The estimated number of deaths ranges from 700,000 to one million (Kidane 1990), with those who experienced the catastrophe in early childhood suffering long-term health consequences into adulthood (Dercon and Porter 2014).
To help Ethiopia cope with the disastrous circumstances, international communities provided a huge amount of emergency aid. International and non-governmental organisations set up relief camps to distribute emergency food and survival items. According to Kurt Jansson, UN Assistant Secretary-General for Emergency Operations in Ethiopia, the relief operation was disturbed by unnecessary bureaucracy, poor road networks, and inadequate transport at the beginning; however, these difficulties were gradually resolved over time (Jansson et al. 1987). Relief camps started to operate as intended mid-1985, lasting until the beginning of 1986. We delve into this 1985 relief operation to study the long-term mitigating impact of emergency aid on health.
Emergency aid as a long-term coping strategy for disasters
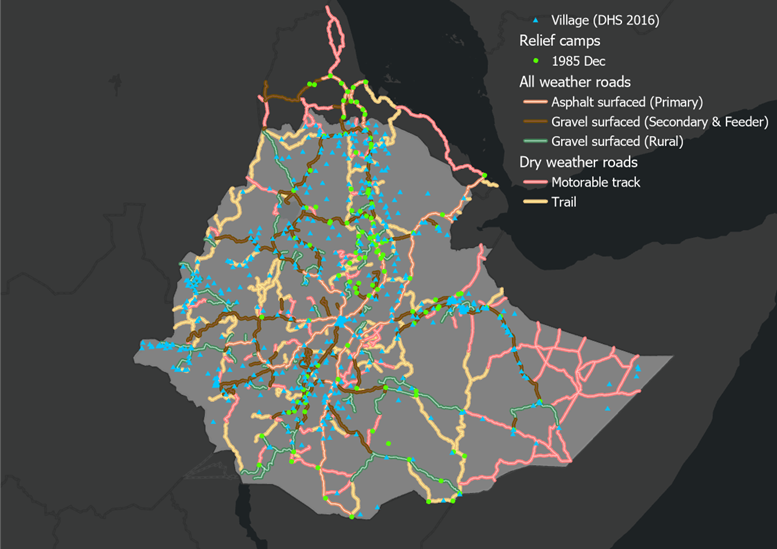
As an indicator of health status in adulthood, we first collect data on adult height measured in the 2016 Ethiopian Demographic and Health Survey (DHS). Second, we digitise the locations of relief camps for the 1985 humanitarian aid operation. Finally, we map the location of villages in DHS onto the geospatial data of relief camps. Figure 1 shows the map of the villages and relief camps. Using this map, we measure the nearest distance to a camp from each village as a proxy for accessibility to relief operations and examine whether access to emergency aid in early life has the mitigating impact on health in later life.
Figure 1: 1985 relief camps and DHS sample villages in Ethiopia
We find that the closer children were born to a relief camp, the taller they are likely to be in adulthood. Children born in a village approximately 3 km away from a camp would be 0.93 cm taller in adulthood than those born in a village 50 km away. This is not a negligible gap since Schultz (2002) highlights that an increase in adult height by 1 cm is associated with an 8-10% increase in wages in Ghana and Brazil.
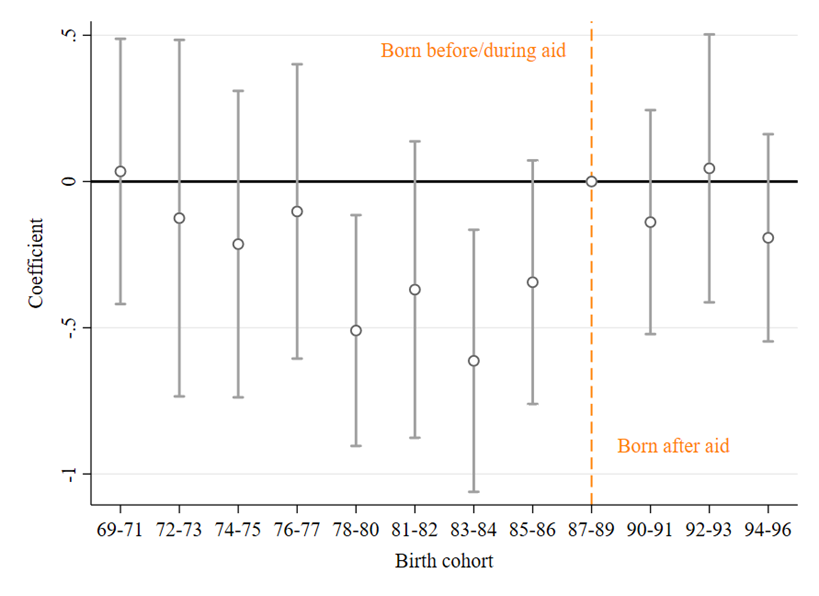
Figure 2 depicts the effects of proximity to a relief camp on adult height by birth cohort. The cohorts born in the 1990s did not benefit from the relief operation (coefficients are close to zero) as they were born after the end of the relief operation. However, the relief operation did have long-term positive impacts on the cohorts born in 1978-86 (i.e. those that were 0-7 years old at the time of relief operation). The negative values of effects imply that adult height increases as the distance to a relief camp from a village of birth decreases. It is also worth noting that the aid effects on the cohorts born before 1978 (i.e., above 7 years old at the time of relief operation) are very small. This suggests that nutritional improvements made after early childhood—the most critical period for growth—are less effective.
Figure 2: The effect of emergency aid on adult height
We also find that the long-term health consequences of emergency aid may translate into gains in labour productivity. Our research shows that the labour productivity (defined as crop yield per working hour) of adults born 3 km away from a camp would be 1.2 times higher than that of adults born 50 km away. This finding provides suggestive evidence that improved health due to access to emergency aid in early childhood contributes to higher labour productivity in adulthood.
Policy implications: We should not underestimate the role of emergency aid
Our findings underscore the importance of emergency aid not only as an immediate but also as a long-term coping strategy for large-scale disasters. We are living in the era of humanitarian crises, but current global efforts for humanitarian funding are in decline (Bruni and Sterck 2025, Husain 2024). Our research suggests that emergency aid serves as a critical buffer, shielding children from the long-lasting consequences of disasters. Recent cuts to humanitarian aid could lead to an intergenerational deterioration of health and socio-economic conditions. The impacts of short-term emergency aid linger longer than we think. The role of emergency aid thus must be acknowledged as a contributor to long-term disaster mitigation as well as temporary assistance.
References
Bruni, V and O Sterck (2025), “What happens when humanitarian aid is cut or delayed?” VoxDev.
Centre for Research on the Epidemiology of Disasters (CRED) (2025), "2024 disasters in numbers."
Cunha, F and J Heckman (2007), “The technology of skill formation,” American Economic Review, 97(2): 31–47.
Dercon, S and C Porter (2014), “Live aid revisited: Long-term impacts of the 1984 Ethiopian famine on children,” Journal of the European Economic Association, 12(4): 927–948.
Di Falco, S and K Han (2025), “Mitigating the health impact of a famine: Evidence from the 1985 Ethiopian emergency food aid,” Journal of Development Economics, 103531.
Dinkelman, T (2017), “Long‐run health repercussions of drought shocks: Evidence from South African homelands,” The Economic Journal, 127(604): 1906–1939.
EM-DAT, CRED/UCLouvain (2024), “Number of recorded natural disaster events, 1900 to 2023.”
Fink, G and S Redaelli (2011), “Determinants of international emergency aid—Humanitarian need only?” World Development, 39(5): 741–757.
Husain, A (2024), “Humanitarian aid and the costs of inaction,” VoxDev.
Jansson, K, M Harris, and A Penrose (1987), The Ethiopian Famine.
Kidane, A (1990), “Mortality estimates of the 1984–85 Ethiopian famine,” Scandinavian Journal of Social Medicine, 18(4): 281–286.
Maccini, S and D Yang (2009), “Under the weather: Health, schooling, and economic consequences of early-life rainfall,” American Economic Review, 99(3): 1006–1026.
Schultz, T P (2002), “Wage gains associated with height as a form of health human capital,” American Economic Review, 92(2): 349–353.