




Adding home visits to a social safety net programme providing cash transfers and parenting information led to sustained improvements in child development, health behaviours, and education outcomes in Burkina Faso, whereas cash alone produced fewer lasting effects.
Cash transfers are a cornerstone of social protection. For decades, government social safety nets have included cash transfers to support poor households in helping their children reach their full potential (Fiszbein and Schady 2009, Bouguen et al. 2019). Yet over 250 million children under age five in developing countries do not reach their full development potential and are less likely to become healthy, productive, and socio-economically successful adults (Grantham-McGregor et al. 2007, Lu et al. 2016, Britto et al. 2017). To address this gap, governments have sought complementary approaches to help children early in life (Draper et al. 2024, Nores et al. 2024), with a growing emphasis on parent-focused early childhood interventions (Doyle 2020). Seminal work evaluating a home visit intervention in Jamaica showed short-term improvements in child development (Grantham-McGregor et al. 1991) and large impacts on adult outcomes decades later (Gertler et al. 2014).
There is, however, limited evidence on whether combining components – such as parenting interventions and cash transfers – into an integrated social safety net is more effective than providing separate interventions, and which specific components drive that effectiveness.
Cash, information meetings, and home visits
In recent work, we present medium-term results from a randomised controlled trial of a government-run integrated social safety net programme operated at scale in Burkina Faso focusing on child development (Akresh, de Walque, Kazianga, and Stocker 2025). Specifically, we seek to understand whether adding parenting-focused interventions on top of a cash transfer programme is effective and whether the delivery mode of the parenting intervention matters. The key components of our intervention include cash transfers, information meetings with small groups of mothers, and home visits. In this work, we aim to determine whether combining these components in an integrated social safety net improves child development and whether these beneficial effects last once the intervention ends.
We conducted a randomised controlled trial in 225 rural villages where villages were randomly assigned to a control group or one of the following treatments: unconditional cash transfers only; unconditional cash transfers plus government-run information meetings focused on child health and psychosocial development; or unconditional cash transfers, information, and home visits reinforcing the information meetings.
Households in all treatment groups received a quarterly cash transfer from the government of approximately US$62, which is around 10.7% of household quarterly food consumption and non-food expenditures. In the treatment groups that included information meetings, government-trained social workers ran monthly village-level information meetings for groups of 25–30 mothers. Finally, in the treatment groups that received home visits in addition to cash and information, these social workers conducted twice monthly home visits to monitor progress and follow up on children’s physical and cognitive development. The curriculum and content for the group information meetings and the home visits were the same, but their delivery mode varied. The cash intervention lasted for 30 months, while the information and home visits lasted for 18 months.
Focusing on health, education, and early childhood development
To measure the intervention’s impact, we conducted a baseline survey prior to the treatment rollout and were scheduled to conduct an endline survey immediately after the intervention ended. However, insecurity in Burkina Faso forced us to delay the endline survey by 15 months, and we were only able to conduct the endline survey in 74 of the villages. Despite these challenges, we were able to maintain balance across the study groups. All results should therefore be interpreted as medium-term impacts after the intervention ended.
In our analysis, we focus on the impacts of cash, information, and home visits on fertility, health behaviours, child anthropometrics, child education, and early childhood development. We administered two early childhood development tests: the Strengths and Difficulties Questionnaire (SDQ) and the Denver Prescreening Developmental Questionnaire.
Home visits strengthen programme impacts
Figure 1 presents the treatment impacts on six different indices that summarise these outcomes. For the cash-only treatment arm, fifteen months after the intervention ended, we see lasting positive impacts but only on the education and Strengths and Difficulties indices. Results are similar, though less statistically meaningful, for the treatment arm that adds information meetings. We see the largest positive lasting impacts when home visits are added to cash plus information meetings. We observe significant impacts on pregnancy, health behaviours, education, and Strengths and Difficulties indices.
Figure 1: Effect of cash, information, and home visits on indices
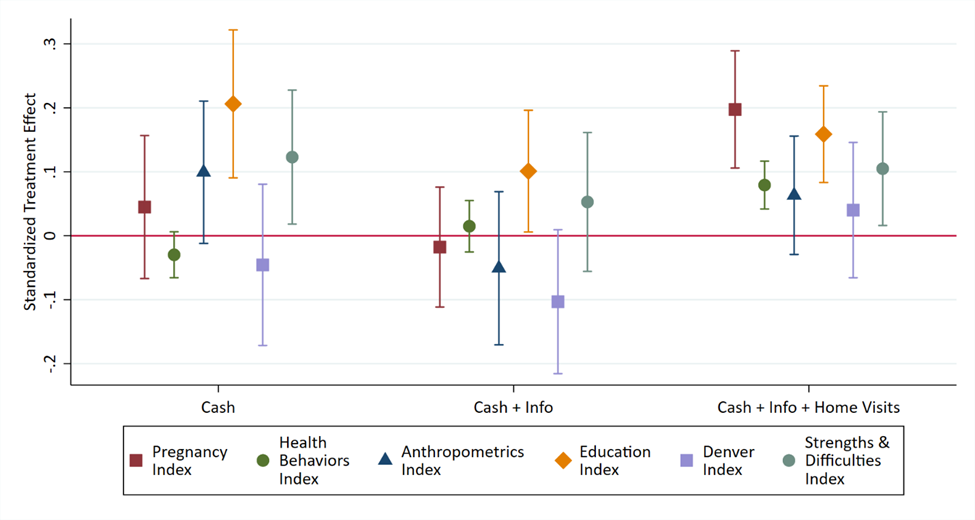
More specifically, households receiving the full integrated social safety net intervention (cash, information, and home visits) experience lasting improvements across a range of outcomes. Mothers have fewer pregnancies and are older at each birth. Their most recent birth is more likely to have been assisted by a health professional. They adopt healthier behaviours, including providing improved nutrition for young children, increasing the use of mosquito bed nets for children, attending more prenatal visits during their most recent pregnancy, and washing their hands more frequently after using the toilet and before meals. Child morbidity also declines. When households receive only cash, or cash combined with information, only a few health behaviours show lasting improvements, with no observed improvements in pregnancy outcomes.
Educational outcomes improve for older children in households receiving the full intervention, including a higher likelihood of school enrolment, more years of school completed, and increased chances of being educationally on track for their age. Similar medium-term effects are observed for households that receive only cash transfers.
The SDQ prosocial scale – reflecting positive social behaviours like helpfulness, consideration, and sharing – exhibits lasting improvements when families received cash, information, and home visits, though Denver test scores were not impacted. Cash and information did not lead to lasting improvements in early childhood development outcomes, highlighting the importance of home visits.
Why is adding home visits so effective?
We conclude from our experiment that adding home visits is essential for enhancing child development, while cash transfers alone produce fewer lasting effects. Why was the combination of cash, information meetings, and home visits so effective? While we cannot measure this directly, we believe that home visits brought salience and accountability to the intervention. Parents felt like the government cared enough about them and their children. Additionally, the same social worker usually visited the same households, building trust and accountability through one-to-one relationships.
Our results and cost-benefit analysis lead us to conclude that adding home visits for households already receiving cash and information is effective and has high marginal returns. This conclusion should encourage policymakers to consider home visits reinforcing parenting and health best practices as an essential tool in social safety nets and in programmes aimed at improving children’s human development potential.
References
Akresh, R, D de Walque, H Kazianga, and A Stocker (2025), “Medium-term impacts of integrated social safety nets: Cash transfers, information meetings, and home visits for child development,” Unpublished manuscript.
Bouguen, A, Y Huang, M Kremer, and E Miguel (2019), “Using randomized controlled trials to estimate long-run impacts in development economics,” Annual Review of Economics, 11: 523–561.
Britto, P, S Lye, K Proulx, A Yousafzai, S Matthews, T Vaivada, R Perez-Escamilla, N Rao, P Ip, L Fernald, H MacMillan, M Hanson, T Wachs, H Yao, H Yoshikawa, A Cerezo, J Leckman, and Z Bhutta (2017), “Nurturing care: Promoting early childhood development,” Lancet, 389(10064): 91–102.
Doyle, O (2020), “The first 2,000 days and children’s skills,” Journal of Political Economy, 128(6): 2067–2122.
Draper, C, A Yousafzai, D McCoy, J Cuartas, J Obradović, S Bhopal, J Fisher, J Jeong, S Klingberg, K Milner, L Pisani, A Roy, J Seiden, C Sudfeld, S Wrottesley, G Fink, M Nores, M Tremblay, and A Okely (2024), “The next 1,000 days: Building on early investments for the health and development of young children,” Lancet, 404(10467): 2094–2116.
Fiszbein, A, and N Schady (2009), "Conditional cash transfers: Reducing present and future poverty," Unpublished manuscript.
Gertler, P, J Heckman, R Pinto, A Zanolini, C Vermeersch, S Walker, S M Chang, and S Grantham-McGregor (2014), “Labor market returns to an early childhood stimulation intervention in Jamaica,” Science, 344(6187): 998–1001.
Grantham-McGregor, S, C Powell, S Walker, and J Himes (1991), “Nutritional supplementation, psychosocial stimulation, and mental development of stunted children: The Jamaican study,” Lancet, 338(8758): 1–5.
Grantham-McGregor, S, Y B Cheung, S Cueto, P Glewwe, L Richter, and B Strupp (2007), “Development potential in the first 5 years for children in developing countries,” Lancet, 369(9555): 60–70.
Lu, C, M Black, and L Richter (2016), “Risk of poor development in young children in low- and middle-income countries: An estimation and analysis at the global, regional, and country level,” Lancet Global Health, 4(12): e916–e922.
Nores, M, C Vazquez, E Gustafsson-Wright, S Osborne, J Cuartas, M Lambiris, D McCoy, F Lopez-Boo, J Behrman, R Bernal, C Draper, A Okely, M Tremblay, A Yousafzai, J Lombardi, and G Fink (2024), “The cost of not investing in the next 1,000 days: Implications for policy and practice,” Lancet, 404(10467): 2117–2130.