





When El Salvador deployed community health teams, the result was not simply more primary care – it was better-organised care, with more prevention, less infectious disease, and fewer patients ending up in hospital for conditions that should never have progressed that far.
Health systems in low- and middle-income countries (LMICs) face a persistent structural problem: too many people seek care for preventable conditions in costly hospitals and emergency rooms, while primary care remains underused. Closing this gap is not simply about building more facilities – it requires reshaping how care is organised and delivered. In recent work (Bancalari, Bernal, Celhay, Martinez, and Sánchez 2026), we examine how El Salvador's nationwide introduction of community health teams (CHTs) – multidisciplinary primary care units deployed across municipalities starting in 2010 – altered the composition of care across all levels of the health system.
The broader context motivates the analysis. Hospital care accounts for roughly 60% of government health expenditure in LMICs (Pinto et al. 2018), and a large share of health spending in high-income countries is considered wasteful (OECD 2017). Prior work has shown that primary care access can reduce avoidable emergency visits and hospitalisations in high-income settings (Kolstad and Kowalski 2012, Alexander et al. 2019, Sabety et al. 2023), but evidence on how reorganising the delivery of primary care affects utilisation across an entire health system in an LMIC is scarce. Research on community health worker (CHW) programmes have documented effects on health outcomes in Brazil (Macinko et al. 2006, Rocha and Soares 2010), Madagascar (Herrera-Almanza and Rosales-Rueda 2023), and South Asia (Barham 2012), but less is known about the mechanisms by which these programmes reshape the mix of preventive and curative care, across different disease burdens, and reduce reliance on costly hospital services.
Bringing health teams to communities
Before the reform, El Salvador's public health system had roughly 377 primary care units serving six million inhabitants, placing substantial pressure on hospital emergency rooms. Primary care was largely inaccessible in rural areas and poorly connected to higher levels of care.
The 2010 reform created government-funded CHTs consisting of physicians, professional nurses, auxiliary nurses, community health workers (CHWs), and support staff. Each team served a defined catchment area – about 3,000 people in rural settings – and was responsible for roughly 300 health services spanning preventive care, curative consultations, and community outreach. A key feature of the model was task-shifting: transferring responsibilities from doctors to nurses and CHWs, thereby lowering the cost of expanding access while preserving quality.
Teams began their work with intensive initial home visits, conducting household hygiene assessments, enrolling the population, and generating health-risk profiles. These visits documented stark conditions: nearly half of households did not treat their drinking water, over 70% lacked proper solid waste management, and disease vectors were present in most homes. Among adults over 50, arterial hypertension, diabetes, and other chronic conditions were widespread – yet largely untreated at the primary level.
Measuring the effects of community health teams
CHTs were rolled out staggered across 186 of El Salvador's 254 municipalities between 2010 and 2013, with 68 municipalities never receiving teams (Figure 1). We exploit this staggered introduction using an event-study design and the imputation estimator of Borusyak et al. (2024), which avoids the bias introduced by traditional two-way fixed effects when treatment effects evolve over time.
Figure 1: Spatial distribution of CHT creation across municipalities
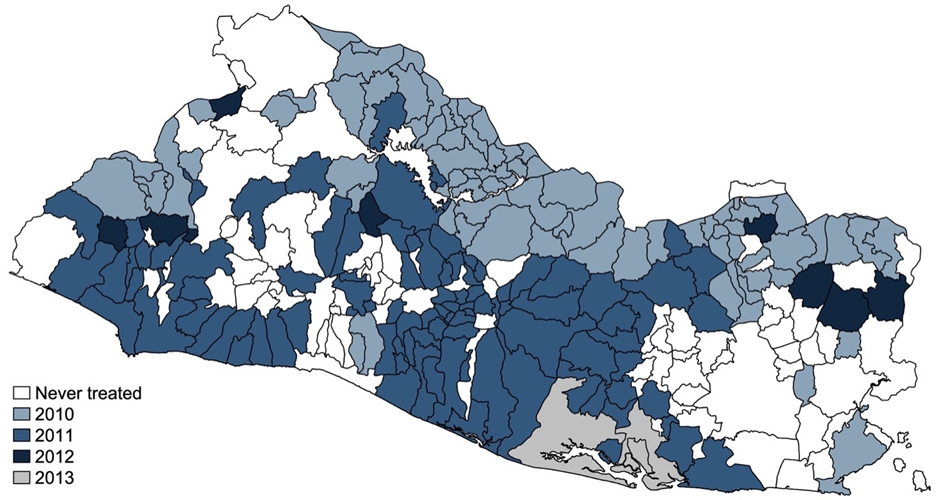
Note: The map shows the year in which CHTs were created, proxied by the year a municipality registered at least 5% of its population into the CHT system.
The dataset combines over 120 million preventive and curative outpatient consultation records (2009–2018) and nearly five million hospital discharge records (2005–2018), aggregated at the municipality–year level. We classified consultations and hospitalisations using ICD-10 codes and established classifications for conditions amenable to primary care – distinguishing communicable diseases (CDs), such as respiratory infections and infectious diseases, from non-communicable diseases (NCDs), such as cardiovascular disease, diabetes, and chronic respiratory conditions.
Community health teams improved care
First, CHTs dramatically expanded preventive care. The average treatment effect on preventive consultations was 187.6 per 1,000 inhabitants – a 37% increase from baseline (Figure 2). The effect was not immediate: in the first year, CHTs substituted home-based health-risk assessments for in-unit preventive checks, and prioritised the highest-risk individuals. From year two onwards, as units reached full operational capacity, preventive consultations rose across all age groups.
Figure 2: Effects on preventive consultations
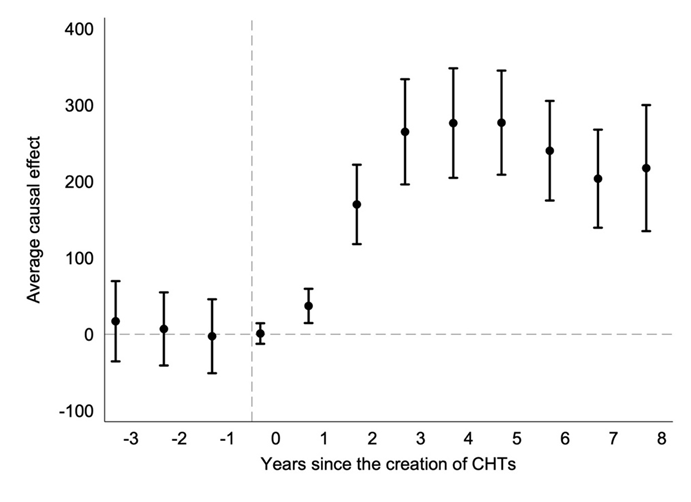
Note: Coefficients from the fully dynamic specification using the Borusyak et al. (2024) imputation estimator. All outcomes measured per 1,000 inhabitants. Confidence intervals at 95%.
Second, CHTs restructured curative care. The net effect on total curative consultations was statistically indistinguishable from zero, but this masks a meaningful reallocation (Figure 3). Amenable curative consultations for communicable diseases fell by 73 per 1,000 inhabitants (8.5%), driven primarily by reductions in respiratory infections, the leading cause of curative visits before the reform. At the same time, curative consultations for NCDs rose by 44.5 per 1,000 inhabitants (17.9%), concentrated among the elderly and driven by cardiovascular disease management – consistent with the chronic conditions CHTs identified as unmet needs during initial home visits.
Figure 3: Effects on amenable curative consultations, by disease type
Panel A: Communicable diseases
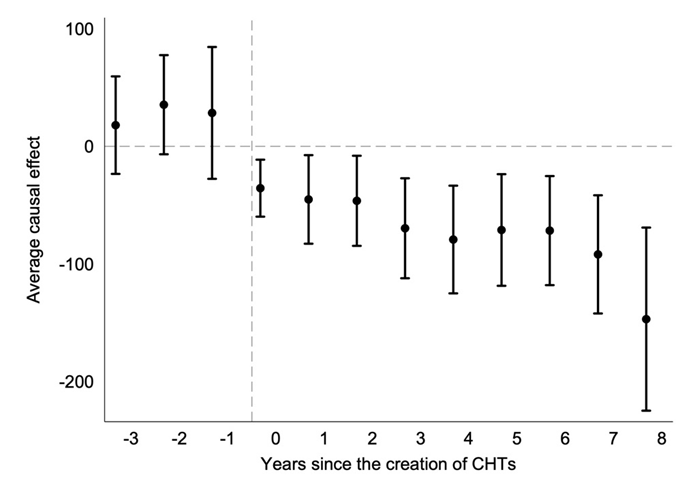
Panel B: Non-communicable diseases
Note: Coefficients from the fully dynamic specification using the Borusyak et al. (2024) imputation estimator. All outcomes measured per 1,000 inhabitants. Confidence intervals at 95%.
This pattern reflects two simultaneous mechanisms: prevention reducing the burden of infectious disease, and newly revealed NCD needs being brought into the care system. Rather than simply generating more visits, CHTs shifted capacity toward higher-need conditions.
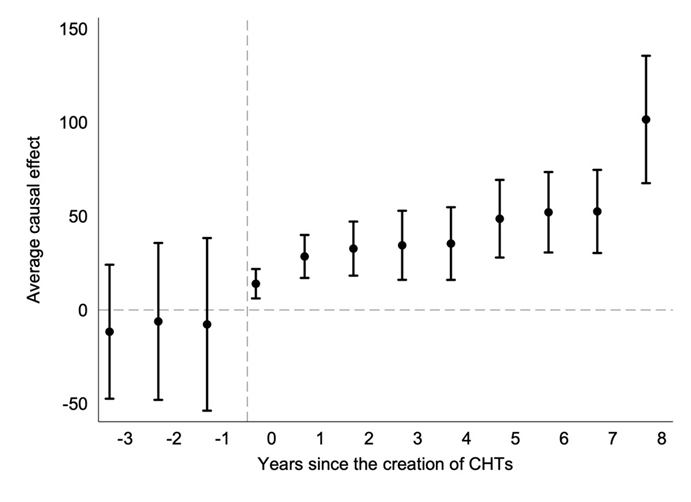
Third, preventable hospitalisations declined. CHTs reduced preventable hospitalisations by 0.8 per 1,000 inhabitants – a 10.8% reduction from the pre-intervention mean. The effect was larger and more precisely estimated for communicable diseases (-13.6%), consistent with the hygiene and infection control activities of CHTs. Reductions in NCD-related hospitalisations were also negative, though less precisely estimated – reflecting that these outcomes depend substantially on behavioural factors such as medication adherence, which are harder to influence (Figure 4). These gains are not driven by a compositional change in overall hospitalisations: the total number of hospital discharges was unaffected, and a placebo test on hospitalisations for external causes (accidents, injury, self-harm) shows no effect.
Suggestive evidence on health outcomes corroborates these utilisation findings: amenable mortality from communicable diseases fell by around 25% following CHT introduction.
Figure 4: Effects on preventable hospitalizations, by disease type
Panel A: Communicable diseases
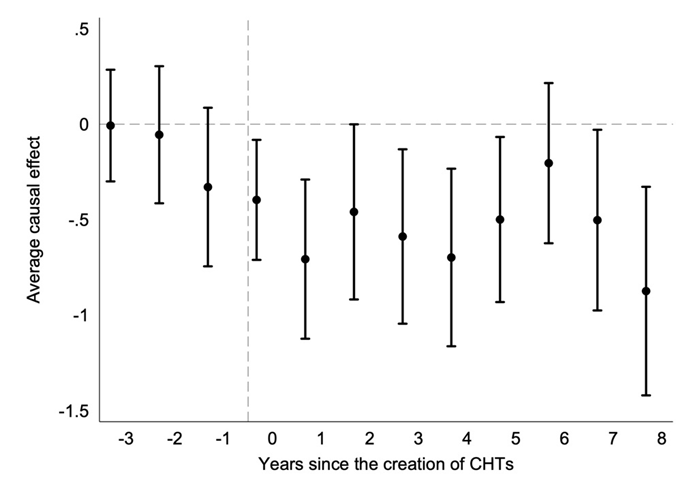
Panel B: Non-communicable diseases
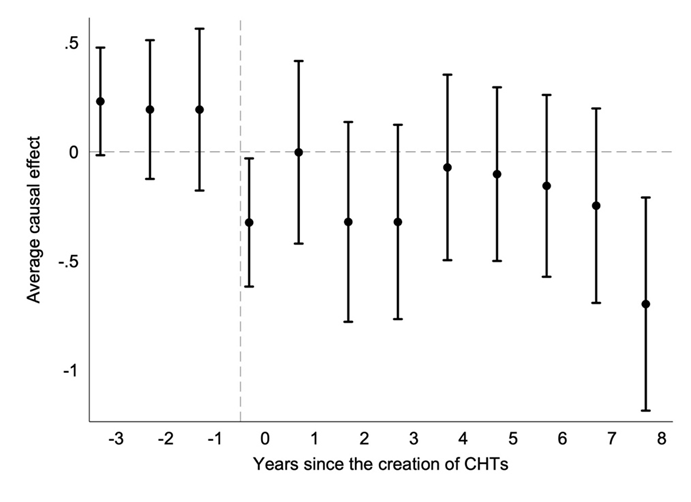
Note: Coefficients from the fully dynamic specification using the Borusyak et al. (2024) imputation estimator. All outcomes measured per 1,000 inhabitants. Confidence intervals at 95%.
What this means for health system design
Several features of the CHT model appear central to these results. The combination of initial home visits and ongoing outreach addressed demand-side barriers – a critical constraint in rural LMICs where populations do not spontaneously access formal care (Dupas 2011). Task-shifting to nurses and CHWs enabled coverage expansion without proportional cost increases in specialist time. Specifically, the reform increased the number of primary care units by 4.1% and total health staff by 10.7%, a rise driven primarily by nurses and support workers rather than doctors (Table 1). This changed the composition of the workforce substantially, with the share of nurses and support workers each rising by around 1–2 percentage points. The initial household census generated actionable targeting: CHTs knew where chronic conditions were going untreated before the first clinic appointment was booked.
Importantly, these results were achieved through a net expansion of health personnel – not reallocation from hospitals. Between 2009 and 2017, physician and nurse density nationally increased from 3.8 to 12.3 per 10,000 inhabitants, with proportionally larger gains at the primary level. This implies that the fiscal cost of the model, while real, bought genuine system-level returns in the form of averted hospital care.
A cost-effectiveness assessment further supports the case for community-based primary care. Using activity-based cost data for El Salvador's health network and disability weights from the Global Burden of Disease study, we estimate the cost per disability-adjusted life year (DALY) averted by CHTs. Relying on our causal estimates – the reallocation of curative consultations and averted preventable hospitalisations – the programme is cost-effective in urban municipalities at roughly US$1,450 per DALY averted, well below El Salvador's GDP per capita threshold of around $5,200. In rural municipalities, where more teams are needed to serve dispersed populations, the estimate is borderline at approximately $4,850 per DALY. Notably, the dominant driver of health gains in this conservative calculation is improved NCD management. These estimates represent a lower bound, as we also find suggestive evidence of a 25% reduction in mortality from communicable diseases amenable to primary care following CHT introduction. This association, if causal, would roughly double the DALYs averted and bring the rural ICER to around $2,300 per DALY, making the programme highly cost-effective across all settings. Together, these results suggest that organised, community-based primary care not only reshapes how care is delivered but also represents good value for money, even before accounting for the full mortality benefit.
Broader lessons for community health in LMICs
El Salvador's experience is not unique in design – Brazil's Family Health Strategy (Macinko et al. 2010) and Costa Rica's EBAIS system share core features, including multidisciplinary teams, home-based outreach, and emphasis on prevention. This research adds large-scale causal evidence that this model can meaningfully shift the composition of care system-wide: increasing prevention, redirecting curative capacity toward chronic disease, and reducing costly and preventable hospitalisations.
For health ministries across Latin America and other LMICs grappling with rising NCD burdens, ageing populations, and persistent inequities in access, these findings speak directly to the value of investing in organised, community-based primary care – not as a substitute for hospital capacity, but as a first-line strategy to use that capacity more efficiently.
References
Alexander, D, J Currie, and M Schnell (2019), "Check up before you check out: Retail clinics and emergency room use," Journal of Public Economics, 178: 104050.
Bancalari, A, P Bernal, P Celhay, S Martinez, and M D Sánchez (2026), "Community health teams and health utilization in El Salvador," Journal of Health Economics, 106: 103110.
Barham, T (2012), "Enhancing cognitive functioning: Medium-term effects of a health and family planning program in Matlab," American Economic Journal: Applied Economics, 4(1): 245–273.
Borusyak, K, X Jaravel, and J Spiess (2024), "Revisiting event study designs: Robust and efficient estimation," Review of Economic Studies, 91: 3253–3285.
Dupas, P (2011), "Health behavior in developing countries," Annual Review of Economics, 3: 425–449.
Herrera-Almanza, C, and M F Rosales-Rueda (2023), "Community-based health programs and child vaccinations: Evidence from Madagascar," World Development, 170: 106322.
Kolstad, J T, and A E Kowalski (2012), "The impact of health care reform on hospital and preventive care: Evidence from Massachusetts," Journal of Public Economics, 96(11–12): 909–929.
Macinko, J, I Dourado, R Aquino, et al. (2010), "Major expansion of primary care in Brazil linked to decline in unnecessary hospitalization," Health Affairs, 29(12): 2149–2160.
Macinko, J, F C Guanais, and M D F M De Souza (2006), "Evaluation of the impact of the Family Health Program on infant mortality in Brazil, 1990–2002," Journal of Epidemiology and Community Health, 60(1): 13–19.
OECD (2017), "Tackling wasteful spending on health."
Pinto, D, R Moreno-Serra, G Cafagna, and L Giles Álvarez (2018), "Efficient spending for healthier lives," in A Izquierdo, C Pessino, and G Vuletin (eds), Better Spending for Better Lives, Inter-American Development Bank.
Rocha, R, and R R Soares (2010), "Evaluating the impact of community-based health interventions: Evidence from Brazil's Family Health Program," Health Economics, 19(S1): 126–158.
Sabety, A, J Gruber, J Y Bae, and R Sood (2023), "Reducing frictions in healthcare access: The Action Health NYC experiment for undocumented immigrants," American Economic Review: Insights, 5(3): 327–346.