


Merit-based recruitment and higher pay in Chile’s public hospitals attracted better-trained managers – leading to lower mortality rates and improved healthcare performance.
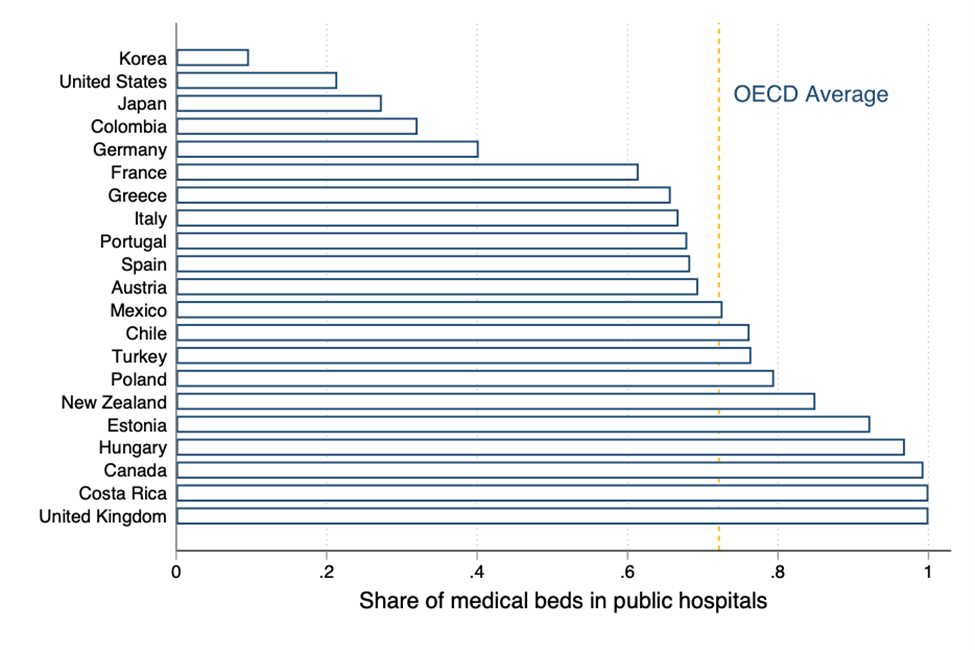
Government spending on publicly provided goods and services has increased substantially over the past 40 years and now accounts for around 30% of global GDP (Gethin 2025). This rise is particularly pronounced in healthcare, where government spending as a share of national income has grown by 60% on average over the same period. Today, the average OECD country allocates nearly one-fifth of its budget to health, with public hospitals delivering most of this care (Figure 1).
Figure 1: Share of medical beds provided by public hospitals in OECD economies
Given the scale of public spending, improving how states deliver goods and services is central to government productivity and development. While scholars have long emphasised the importance of bureaucratic capacity (Wilson 1989, Evans and Rauch 1999) and the role of managerial quality (Pollitt and Bouckaert 2017), there is limited causal evidence on whether better managers actually improve public provision. Do higher-quality managers raise service quality and can reforms to hiring and pay systems help attract them? Our research (Muñoz and Otero 2025) addresses these questions by analysing a major senior civil service reform in Chile that introduced competitive recruitment for top managers of public hospitals: CEOs.
A reform triggered by scandal
In 2003, a political scandal over illegal payments to government officials prompted Chile’s Congress to enact a sweeping civil service reform. The new framework created a Senior Executive Service system designed to ensure that top public managers are recruited through open and merit-based processes. The reform also raised base salaries – by around 25% for hospital CEOs – in order to make these positions more competitive with the private sector.
Importantly, the reform was rolled out gradually: some hospitals adopted the new rules as early as 2005, while others did so only years later. This staggered adoption created a natural experiment, allowing us to identify the causal impact of competitive recruitment.
Studying the impact of civil service reform in Chile’s public hospitals
To measure a wide range of outcomes, we assembled a novel dataset from multiple sources. We collected detailed information on CEO careers and education through hundreds of Freedom of Information Act requests and archival work. We complemented this with hospital workforce records that captured wages and turnover, patient-level data covering 16.5 million inpatient discharges from all Chilean public hospitals, and national death registry records that included both in-hospital and post-discharge deaths.
There were fewer deaths after the reform
Exploiting the staggered rollout of the reform across hospitals, we estimate a difference-in differences model and find that hospital mortality dropped significantly after the adoption of the new hiring system. In-hospital death rates decreased by 8% in the three years following the reform (Figure 2), which corresponds to two fewer deaths per 1,000 patients, from the pre-reform baseline of 2.6%. We also document significant improvements among emergency and non-deferrable admissions, where timely and coordinated management is especially crucial. The reduction in mortality remains robust when using alternative measures, such as 28-day mortality and risk-adjusted death rates.
Figure 2: Dynamic effects of the reform on hospital quality
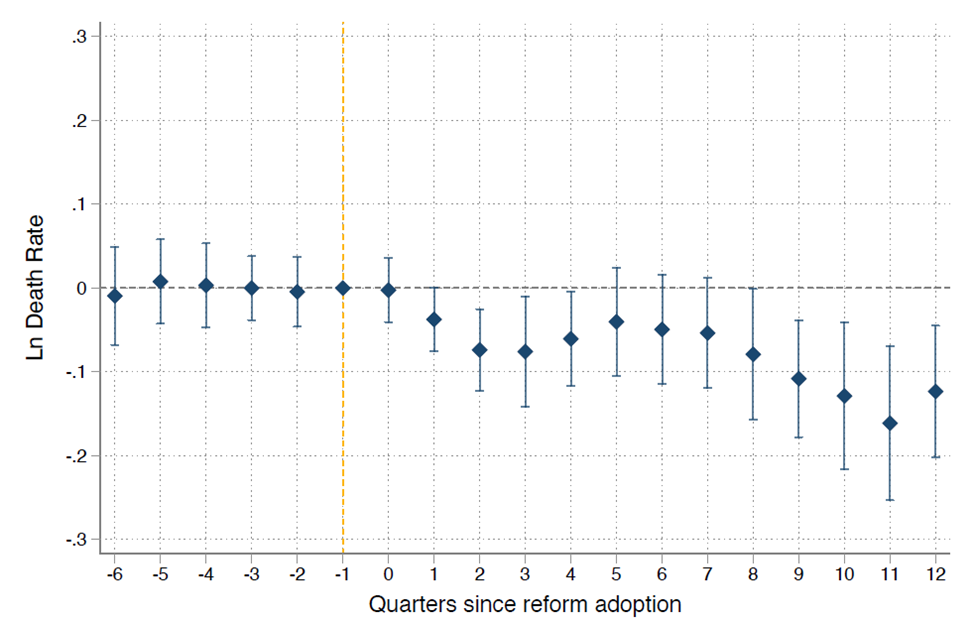
Importantly, the reduction in mortality was not driven by changes in patient composition. Chilean public hospitals cannot legally select patients, and we find no evidence of shifts in case mix, spillovers to neighbouring hospitals, or increases in home deaths. Instead, we find that the reform reduced doctor turnover, suggesting that better-managed hospitals were more successful at retaining highly skilled personnel.
Why managers matter
What accounts for these improvements? We show that managers themselves play a key role in hospital performance. CEO identity accounts for a substantial share of the variation in mortality: adding CEO fixed effects increases the share of explained variance in the in-hospital death rate, which is our measure of performance. This increase in the explained variance is comparable to that found in research on the role of managers in US firms (Bertrand and Schoar 2003) and Italian public agencies (Fenizia 2022). In our setting, when a high-talent CEO arrives, mortality falls, and when one departs, it rises – with the opposite effects observed for the arrival and departure of low-talent CEOs.
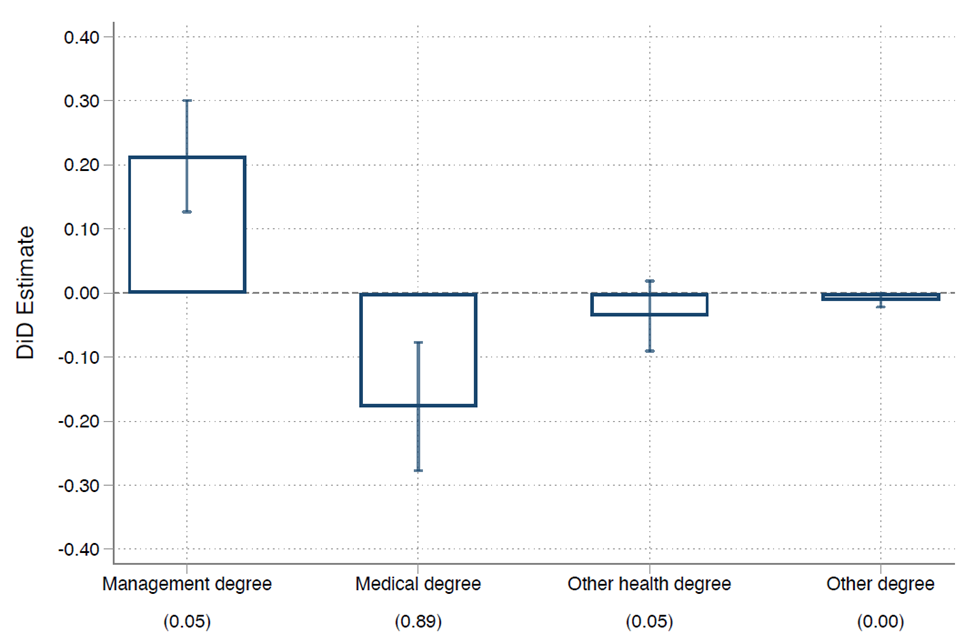
We then turn to the mechanisms, focusing on how the reform reshaped who became CEOs. Before the senior civil service reform, virtually all hospital CEOs were doctors: in 2004, 99% held medical degrees. The reform changed this social norm, and raised the share of non-doctor CEOs with management degrees by more than 20 percentage points (Figure 3). By the end of our analysis period in 2019, only around half of CEOs were doctors. An important finding is that the reform displaced only doctor CEOs with no management training and actually increased the share of doctor CEOs with postgraduate management training by around 15 percentage points. Taken together, the reform increased the likelihood that a hospital CEO had either an undergraduate or postgraduate degree in management by 36 percentage points, up from the pre-reform average of 28%. For comparison, only around 26% of public hospitals CEOs in England have postgraduate management training (Janke et al. 2018), and across hospitals in nine countries, roughly one-quarter of managers report having similar training (Bloom et al. 2020).
Figure 3: The policy displaced doctor CEOs with no management training
Finally, we investigate if post-reform CEO characteristics explain the observed improvements in performance. Our analysis shows that the gains were concentrated in hospitals that hired higher-quality managers, as measured by their CEO fixed effects. Interestingly, in terms of observable CEO characteristics, formal management training is the best predictor of post-reform performance. We find no performance differences between doctor and non-doctor CEOs once both possess formal management training.
A closer look at pay incentives
The reform also raised CEO pay by around 25%. This pay increase may have attracted higher-ability CEOs to apply and also motivated selected CEOs to work harder. To test whether the improvements reflected higher effort in response to increased salaries, we examine several scenarios. First, we ask whether hospitals improved their performance in the few cases where the incumbent manager was reappointed. We find no effect. Second, we examine CEOs who led hospitals in both the pre- and post-reform periods and find that their performance did not differ between the two periods. Finally, we leverage a later amendment that increased pay only for doctor CEOs, which boosted salaries but we find no effect on performance.
Taken together, these results indicate that the reform’s impact came from changes in the identity of the manager rather than greater effort. We hypothesise that higher wages likely helped attract a stronger applicant pool – consistent with evidence that financial incentives can improve the selection of talent into public service (Dal Bó et al. 2013).
Policy implications for public service delivery
Our findings offer important lessons for countries seeking to strengthen their public sectors. Merit-based recruitment and adequate compensation can help attract more talented managers into public service. At the same time, entrenched professional norms may constrain performance. In Chile, hospitals had long been led almost exclusively by doctors, even though a good doctor does not necessarily make a good manager. Breaking this norm improved outcomes – a dynamic that may also be relevant for other public-sector organisations, such as school districts, police forces, and public agencies more broadly.
Although our analysis focuses on Chile, the implications are broader. Many low- and middle-income countries are expanding public services but struggle with bureaucratic effectiveness. The Chilean reform shows that strengthening the quality of public managers can deliver measurable improvements in citizens’ lives, even in high-stakes sectors such as health.
References
Bertrand, M and A Schoar (2003), “Managing with style: The effect of managers on firm policies,” Quarterly Journal of Economics 118(4): 1169–1208.
Bloom, N, R Lemos, R Sadun, and J Van Reenen (2020), “Healthy business? Managerial education and management in health care,” Review of Economics and Statistics 102(3): 506–517.
Dal Bó, E, F Finan, and M A Rossi (2013), “Strengthening state capabilities: The role of financial incentives in the call to public service,” Quarterly Journal of Economics 128(3): 1169–1218.
Evans, P and J E Rauch (1999), “Bureaucracy and growth: A cross-national analysis of the effects of ‘Weberian’ state structures on economic growth,” American Sociological Review 64(5): 748–765.
Fenizia, A (2022), “Managers and productivity in the public sector,” Econometrica 90(3): 1063–1084.
Gethin, A (2025), “Revisiting global poverty reduction: Public services and the world distribution of income, 1980–2022,” Unpublished manuscript.
Janke, K, C Propper, and R Sadun (2018), “The impact of CEOs in the public sector: Evidence from the English NHS,” Unpublished manuscript.
Muñoz, P and C Otero (2025), “Managers and public hospital performance,” American Economic Review 115(11): 4040–4074.
Pollitt, C and G Bouckaert (2017), Public management reform: A comparative analysis – Into the age of austerity (4th ed.), Oxford University Press.
Wilson, J Q (1989), Bureaucracy: What government agencies do and why they do it, Basic Books.