





Face-to-face counselling for Nepali adolescents improved mental well-being, but translating these gains into better schooling outcomes proved elusive.
Adolescent mental health is an urgent global concern: one in seven youths aged 10-19 suffers from a mental disorder, yet most go untreated (Currie 2025, WHO 2024). The challenge is particularly acute in low-income countries, where stigma, limited awareness, and insufficient infrastructure severely restrict access to mental health care. In Nepal, mental health issues among adolescents are frequently overlooked due to social stigma and lack of resources; the country’s first specialised child psychiatry clinic only opened in 2015, with virtually no services available outside the capital (Raj 2024). Neglecting mental health may carry significant long-term costs, including impaired physical health, disrupted education, and reduced future economic opportunities. In contrast, improved mental well-being is linked to greater human capital investment (Baranov et al. 2020), enhanced pro-social behaviour (Blattman et al. 2017), and higher lifetime earnings (Lund et al. 2024, Ridley et al. 2020). However, much of this evidence pertains to adult populations, leaving a critical gap in our understanding of which interventions are effective for younger individuals. This underscores an urgent policy question: how can we effectively deliver mental health care to adolescents in low-resource environments?
Talk therapies have proven effective for adolescents in high-income contexts (Weisz et al. 2017), but significant gaps remain in adapting them for low-income settings. First, traditional therapies typically require clinical diagnoses, but formal mental health screening is rare in poor communities. Identifying adolescents needing support without established referral systems or trained professionals is challenging, and little evidence exists on the effectiveness of teacher or community referrals. Second, stigma raises questions about demand and uptake (Lacey et al. 2024). Policymakers worry adolescents or their families may refuse or discontinue therapy due to social taboos surrounding mental illness. Third, human resources pose substantial constraints. Given the severe shortage of mental health professionals in low-income countries, therapy must often rely on trained lay counsellors or school-based delivery. While recent evidence shows promise for school-based life skills classes to improve child socioemotional well-being (Andrew et al. 2022, Baird et al. 2025, Dinarte and Egana-delSol 2024, Edmonds et al. 2020), it remains important to study individualised face-to-face therapy, as group-based approaches may not adequately address the specific needs of adolescents needing more targeted psychological support.
A tailored talk therapy programme for at-risk Nepali youth
To investigate the feasibility of individualised therapy in a resource-poor setting, we conducted a large randomised controlled trial in Nepal (Edmonds et al. 2025). Partnering with a Nepali mental health NGO, we offered free one-on-one face-to-face therapy to adolescents identified by local teachers as being at risk of school dropout. No formal clinical diagnosis was required, recognising that many distressed youths in such environments remain undiagnosed. Leveraging teachers’ insights helped us reach adolescents otherwise overlooked by the health system.
Participants received four weekly hour-long sessions, with the option of two additional private sessions from trained counsellors, tailored to their individual needs. Sessions typically addressed anxiety, depression, bullying, family conflict, and stress management. In addition, counsellors also conducted two separate family therapy sessions involving adolescents and caregivers together. All sessions took place over approximately two months, usually at home. The therapy used relatable stories, role-playing, and smartphone-based materials to engage adolescents and build coping skills. Crucially, families incurred no cost.
Our research involved 1,707 adolescents (aged 13-18) from 40 government schools in seven relatively poor urban and semi-urban municipalities, making it one of the largest therapy trials for youth in a developing country. By embedding the intervention within schools and partnering with a local organisation, the programme leveraged existing community structures, offering a potentially scalable model if effective.
The high uptake of the therapy programme suggests stigma can be overcome
Demand for the programme was very high: 89% of offered students attended at least one counselling session. Such a high take-up rate is encouraging, especially given concerns that stigma or low awareness might lead to low participation. In fact, many students completed the full course of therapy: 82% of those who started attended at least the four core sessions, and the vast majority of their parents or guardians (94%) also engaged in the family sessions.
Figure 1: Take-up and the age distribution of subjects assigned to therapy
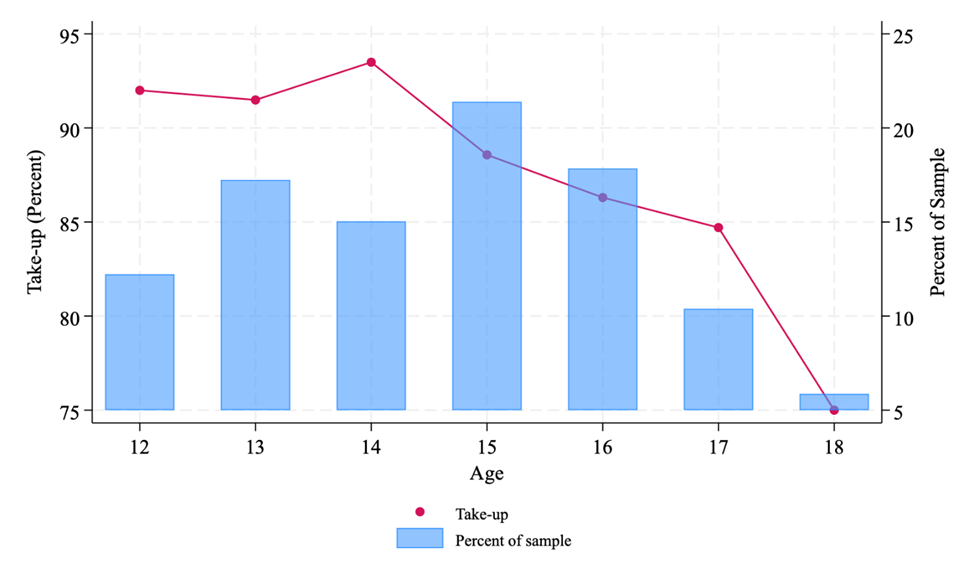
Notes: For the 818 subjects assigned to therapy, the blue bars are a histogram of the age distribution of the population. The red line depicts the percent of subjects at each age that ever participate in any therapy sessions.
Interestingly, younger subjects were more likely to take up the offer and complete all sessions than older subjects. Older children may value their autonomy more and be more socially aware, which can increase concerns about stigma. Regardless, the overall willingness to engage in counselling was very high across the board.
It appears that if services are easily accessible and free, we can expect uptake among adolescents to be high. Teachers likely played a key role in encouraging participation. As trusted figures, their referrals may have reassured students and parents that the therapy was credible and worthwhile. Moreover, by not requiring a formal diagnosis or label, the programme perhaps avoided stigma–subjects were invited because they were having some difficulties at school, which can be a more acceptable reason than being labelled ‘mentally ill’. The high uptake in our study shows that, with thoughtful delivery, stigma is not an insurmountable barrier.
Therapy improved mental health across a broad group of adolescents
Engaging in the therapy had meaningful positive impacts on adolescents’ mental health. Figure 2 contains our estimates of the impact of random assignment induced therapy on psychological distress, anxiety, depression, and parent (caregiver) assessment of the child’s psychological distress. All indexes are standardised relative to the control group at the endline.
Figure 2: Impact of therapy on mental health
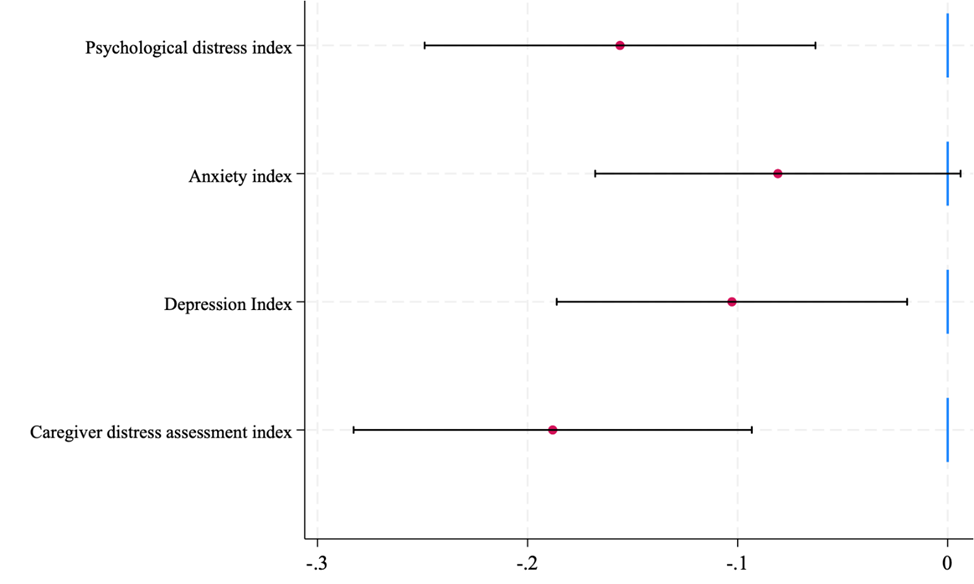
Notes: Each point represents the 2SLS estimate of the effect of randomisation-induced participation in any therapy, controlling for strata fixed effects. 90% confidence intervals pictured. All outcome variables are standardised indexes with a mean of zero and variance of one in the control group. N=1635 for anxiety and depression. N=1488 for the caregiver assessment and the overall psychological distress index (which combines anxiety, depression, and caregiver assessment).
The improvement in overall mental health was moderate in size–roughly a 0.16 standard deviation reduction in distress for the treated on average with a slightly larger effect on depression-associated symptoms compared to anxiety-associated symptoms. Caregivers also noticed these mental health improvements.
These self-reported improvements in mental health appear to be driven by subjects feeling less afraid for the future and reporting fewer sleep problems. Parents emphasise that their child appears less down and better able to manage worries. The consistency between youth and caregiver reports gives us more confidence that these mental health gains were real and perceptible in daily life. These specific questions reflect a general pattern in responses. Emotional regulation – the ability of youths to manage their emotions and cope with stress – improved, and their outlook on life became more positive (an improvement of 0.08 standard deviations in an index of optimism and future expectations). Though generally not statistically significant, we also see general improvements in social relationships with parents and friends.
Crucially, these improvements were achieved among a broad group of adolescents without requiring a clinical diagnosis. This challenges the traditional focus on only treating diagnosed cases.
Therapy was not a quick fix for educational outcomes
While the therapeutic intervention clearly boosted adolescents’ mental health, these psychological gains did not automatically translate into better educational outcomes, at least in the short run. We tracked school attendance records and administered digit-span tests to see if counselling helped students re-engage with school or improve their cognitive skills.
Figure 3: Impact of therapy on school attendance and digit span cognitive tests
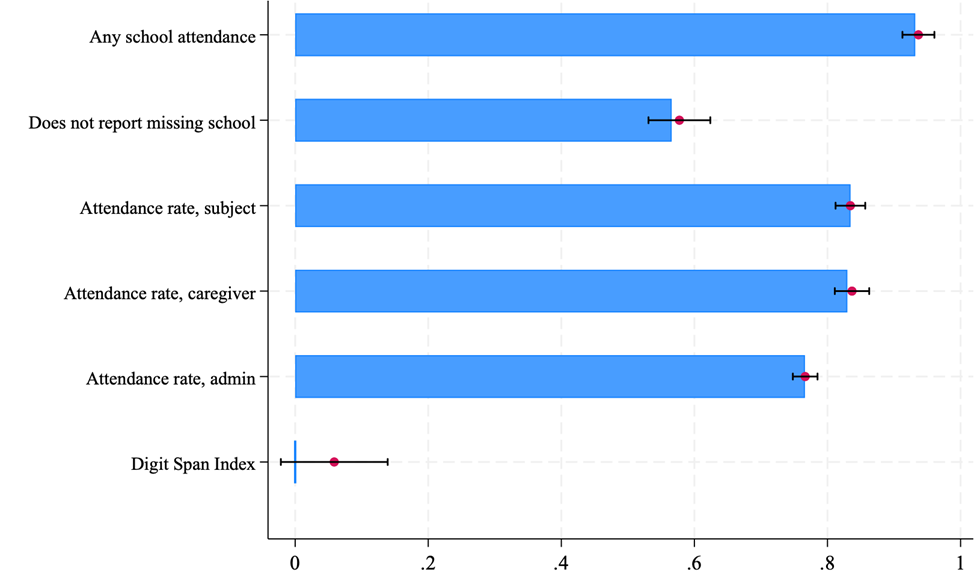
Notes: The coefficient and 90% confidence intervals follow the same econometric approach as Figure 2. N = 1,635 subject responses although there are two missing responses for “does not report missing school” and eight missing responses for “attendance rate, subject” are participants with endline consent and non-missing observations for subject reported variables. N=1507 for caregiver reports. N=1048 for school records. The digit span index test is available only for in-person surveys (N=1,540).
Our results show no significant effects on school attendance rates or cognition, tempering the hope that improving mental health alone would boost human capital accumulation. Many of the adolescents in our sample were struggling in school or contemplating dropping out prior to the intervention. We had hypothesised that by alleviating their distress, improving self-esteem, and resolving personal challenges, therapy might help them refocus on academics. Yet, at least over the period we observed, counselling by itself was not enough to get better educational traction. It is plausible that academic outcomes take longer to materialise – mental health improvements may need more time to translate into concentration, effort, and ultimately grades. It is possible that given another year, some educational benefits may emerge (for example, if a happier student is less likely to drop out in the next grade). Another theory is that structural barriers remained: poverty and household responsibilities, for instance, may still pull these adolescents away from school, regardless of their improved mindset. Therefore, a key takeaway is that mental health interventions can improve welfare (a worthy goal in itself) even if they do not immediately improve academic outcomes.
Lessons for scaling up adolescent mental health care
Our experience in Nepal offers several lessons for designing and scaling mental health services for adolescents in low-resource settings. First, accessibility is crucial. By bringing counselling to families and involving teachers and families, the programme overcame many traditional barriers. This model – integrating mental health support into existing community institutions like schools – could be a cost-effective way to reach youths at scale. Second, it is crucial to normalise mental health care and reduce stigma in the community. Our programme did this implicitly by treating counselling as just another support service for students, akin to academic coaching. Third, the lack of impact on educational outcomes signals that mental health interventions should be seen as complements, not substitutes, to other development interventions. Just as a healthy mind may struggle in a failing school system, an improved school environment may not necessarily help a student who is depressed. Integrated approaches are likely needed. Finally, this intervention underscores the importance of continued innovation and evaluation in mental health service delivery. The positive outcomes we observed came from a relatively intensive, individualised therapy delivered by professional counsellors at a cost of USD$84 per beneficiary. Going forward, testing even lower-cost delivery models may be important: for example, can trained paraprofessionals, peer mentors, or digital platforms deliver group therapy sessions that achieve similar gains? Adapting these ideas for adolescents and rigorously testing them in low-income settings will be vital to inform future policy.
References
Andrew, A, S Krutikova, G Smarrelli and H Verma (2022), “Gender norms, violence and adolescent girls’ trajectories: Evidence from a field experiment in India,” VoxDev.
Baird, S, B Özler, C Dell’Aira, L Parisotto and D Us-Salam (2025), “Therapy, mental health, and human capital accumulation among adolescent girls in Uganda,” Journal of Development Economics, 103473.
Baranov, V, S Bhalotra, P Biroli and J Maselko (2020), “Maternal depression, women’s empowerment, and parental investment: Evidence from a randomized controlled trial,” American Economic Review, 110(3): 824–859.
Blattman, C, J C Jamison and M Sheridan (2017), “Reducing crime and violence: Experimental evidence from cognitive behavioral therapy in Liberia,” American Economic Review, 107(4): 1165–1206.
Currie, J (2025), “Investing in children to address the child mental health crisis,” Unpublished manuscript.
Dinarte, L and P Egana-DelSol (2024), “Combatting school-based violence and nurturing hope in El Salvador,” VoxDev.
Edmonds, E, B Feigenberg and J Leight (2020), “The impact of school-based life skills classes for adolescent girls in India,” VoxDev.
Edmonds, E, P Mukherjee, N Prakash, N Prakash and S Sabarwal (2025), “Talk therapy and human capital in adolescence: Evidence from a low-resource setting,” Unpublished manuscript.
Lacey, L, N Mishra, P Mukherjee, N Prakash, N Prakash, D Quinn, S Sabarwal and D Saraswat (2025), “Can destigmatizing mental health increase willingness to seek help? Experimental evidence from Nepal,” Journal of Policy Analysis and Management, 44: 97–124.
Lund, C, K Orkin, M Witte, J H Walker, T Davies, J Haushofer, S Murray, J Bass, L Murray, W Tol et al. (2024), “The effects of mental health interventions on labor market outcomes in low- and middle-income countries,” Unpublished manuscript.
Raj, A (2024), “Nepal unprepared to tackle children’s mental health problems,” The Kathmandu Post.
Ridley, M, G Rao, F Schilbach and V Patel (2020), “Poverty, depression, and anxiety: Causal evidence and mechanisms,” Science, 370(6522).
Weisz, J R, S Kuppens, M Y Ng et al. (2017), “What five decades of research tells us about the effects of youth psychological therapy: A multilevel meta-analysis and implications for science and practice,” American Psychologist, 72(2): 79–117.
World Health Organization (WHO) (2024), “Mental health of adolescents”.