




Reserving seats for women in parliament leads to sharp reductions in maternal mortality in low- and middle-income countries
Maternal deaths are estimated to account for 830 deaths per day and more than 216 deaths per 100,000 live births globally (Ceschia and Horton 2016). Even with sharp declines in the last two decades, high rates of maternal mortality persist, which is striking given that the knowledge and low-cost technologies needed to dramatically reduce it have been available for nearly a century (Cutler et al. 2006, Loudon 1992). Differential adoption of these technologies may help explain why some countries have experienced dramatic declines in maternal mortality, while others have demonstrated little progress. But why do countries fail to adopt these technologies in the first place?
The importance of political will
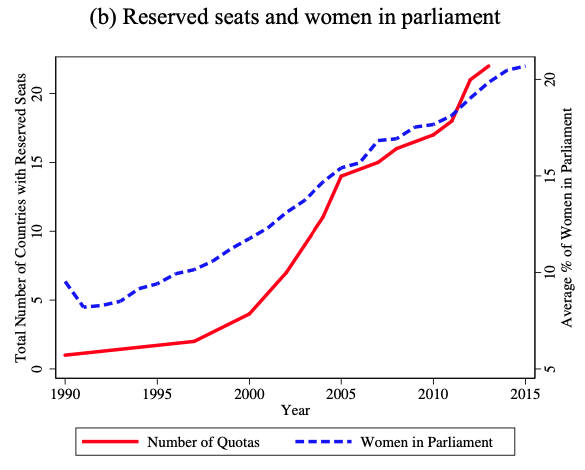
In our recent working paper (Bhalotra et al. 2020), we highlight the relevance of political will, investigating whether female policymakers are more likely to prioritise the reduction of maternal mortality. Between 1990 and 2015, maternal mortality ratios (MMRs), defined as the number of maternal deaths per 100,000 live births, fell by 44%. In this same time period the share of women in parliament across the world doubled from 10% to 20%, as depicted in Figure 1a. Establishing a causal relationship is challenging as the share of women in parliament has increased at a smooth rate, making it hard to isolate its effects from those of other gradually evolving trends. However, the last few decades have seen 22 countries abruptly introduce legislation on parliamentary gender quotas, as shown in Figure 1b. This acts a natural experiment, allowing us to gain a measure on causality.
Figure 1 Trends in gender quotas, women in parliament and maternal mortality

Gender quotas and maternal mortality
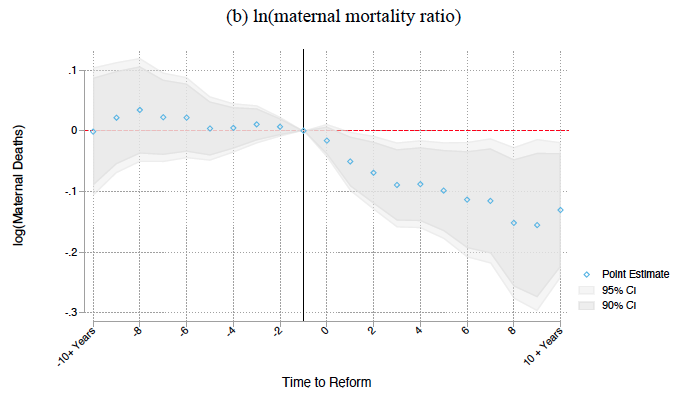
Combining country-specific dates of adoption of gender quotas reserving seats for women in parliament, with data on MMRs across countries, we are able to pinpoint an important causal relationship. Our estimates demonstrate that passage of parliamentary gender quotas leads to an immediate five to six percentage point increase in the share of parliamentary seats held by women. Importantly, this is followed by a 9-12% decrease in the maternal mortality ratio, as shown in Figure 2 below.
Crucially, the pre-legislation trend in MMRs in countries adopting quotas is similar to that in countries not adopting quotas. This suggests that our estimates are not biased by quota-adopting countries starting to address the MMR before the quota was legislated. This makes it easier to ascribe the observed decline in the MMR to quotas. Moreover, we find that gender quotas cause larger declines in the MMR the longer they have been in place, and the larger the share of seats reserved for women.
Figure 2 Gender quotas: Event studies for women in parliament and maternal mortality

Explaining the role of quota adoption in reducing maternal mortality
Our results are consistent with a growing body of evidence that suggests women policymakers are effective in agenda-setting and coalition building, leading to greater parliamentary focus on women’s health issues (Asiedu et al. 2018, Bhalotra and Clots-Figueras 2014, Clayton and Zetterberg 2018, Lippmann 2019, Miller 2008). In particular, we find evidence of increasing investments in key low-cost medical inputs. Gender quotas result in an 8.3–9.8% increase in skilled birth attendance and a 6.2–11.8% increase in antenatal care utilisation. The WHO recommends universal access to these inputs, and they are widely promoted as tools for maternal mortality reduction (WHO 2014, Jamison et al. 2013).
We also find a 4–10% decline in birth rates and an increase in girls’ education of 0.6 years following gender quotas, both of which previous research has shown to be associated with lower maternal mortality (Tressel and Pebley 1984, Bhalotra and Clarke 2013). Importantly, we find no evidence that quotas led to increases in GDP or in receipt of international developmental assistance for women’s health. This suggests that women act on MMR reduction not so much through raising additional resources, but rather through influencing the allocation of resources.
Women parliamentarians prioritise women’s health
We find no significant impact of quotas on adult male mortality, a crude analogue of maternal mortality. Further, we see no impact of quotas on tuberculosis mortality, a highly prevalent disease in low-income countries that mostly affects adults in their (re)productive years and is equally burdensome for men and women. However, we find some evidence that gender quotas result in a fall in infant mortality for girls, but not boys. Combining all of this evidence suggests that women parliamentarians prioritise women’s health.
Policy implications: Ensure women are part of policy decision-making
Efforts to reduce maternal mortality in the last three decades have focused on raising access to trained birth assistance, prenatal and antenatal care, contraception, and women’s education. These efforts have typically focused on calls to raise spending on maternal health. Yet, there has been little recognition among policymakers of the potential relevance of political economy in determining how maternal health investments are prioritised.
Our findings, shared in Bhalotra et al. (2020), suggest that ensuring women are part of the policy decision-making process can lead to dramatic reductions in maternal mortality of the order of 10%. Beyond reducing MMR, research has shown that parliamentary gender quotas have positive impacts on infant health outcomes, and women’s education and empowerment (Baskaran et al. 2018, Bhalotra and Clots-Figueras 2014, Beamen et al. 2012). This, coupled with their budget neutrality, suggests that gender quotas should be seriously considered as an important part of the public health armamentarium going forward.
References
Asiedu, E, C Branstette, N Gaekwad-Babulal and N Malokele (2018), "The effect of women’s representation in parliament and the passing of gender sensitive policies", in ASSA Annual Meeting (Philadelphia, 5-7 January).
Baskaran, T, S Bhalotra, B Min and Y Uppal (2018), “Women legislators and economic performance", IZA Discussion Papers 11596, Institute of Labour Economics, Bonn.
Beaman, L, E Duflo, R Pande and P Topalova (2012), "Female leadership raises aspirations and educational attainment for girls: A policy experiment in India", Science 335(6068): 582-586.
Bhalotra, S, D Clarke, J Gomes and A Venkataramani (2020), “Maternal mortality and women's political participation”, CEPR Discussion Paper 14339.
Bhalotra, S and I Clots-Figueras (2014), “Health and the political agency of women”, American Economic Journal: Economic Policy 6(2): 164-197.
Bhalotra, S and D Clarke (2013), “Educational attainment and maternal mortality”, UNESCO Background paper prepared for the Education for All Global Monitoring Report 2013/4, 2014/ED/EFA/MRT/PI/14.
Ceschia, A and R Horton (2016), “Maternal health: Time for a radical reappraisal”, The Lancet 388(10056): 2064–2066.
Clayton, A and P Zetterberg (2018), “Quota shocks: Electoral gender quotas and government spending priorities worldwide”, The Journal of Politics 80(3): 916-932.
Cutler, D, A Deaton and A Lleras-Muney (2006), “The determinants of mortality”, Journal of Economic Perspectives 20(3): 97–120.
Jamison, D, L Summers, G Alleyne, K Arrow, S Berkley, A Binagwaho, F Bustreo, D Evans, R Feachem, J Frenk, G Ghosh, S Goldie, Y Guo, S Gupta, R Horton, M Kruk, A Mahmoud, L Mohohlo, M Ncube, A Pablos-Mendez, S Reddy, H Saxenian, A Soucat, K Ulltveit-Moe, G Yamey (2013), “Global health 2035: A world converging within a generation”, The Lancet 382(9908): 1898-1955.
Lippman, Q (2019), “Gender and lawmaking in the time of quotas”, Social Science Research Network.
Loudon, I (1992), Death in childbirth: An international study of maternal care and maternal mortality 1800–1950, Clarendon Press.
Miller, G (2008), “Women's suffrage, political responsiveness, and child survival in American history”, The Quarterly Journal of Economics 123(3): 1287-1327.
Tressel, J and A Pebley (1984), “The potential impact of changes in fertility on infant, child and maternal mortality”, Studies in Family Planning 15(6): 267-280.
World Health Organisation (2014), “Maternal mortality”.