



Outsourcing the management of public hospitals in Brazil to private operators increased hospital output and productivity without harming quality or equity, expanding access and reducing mortality, with the gains depending critically on the managerial capacity of the organisations in charge.
Editor's note: The authors have made slides available here.
Governments around the world are increasingly turning to private providers to deliver public services, hoping that private management will boost efficiency and expand access. But economic theory has long warned of trade-offs. Private providers with control over revenues and profits have stronger incentives to innovate and cut costs, which can improve performance (Hart and Moore 1990). Yet when contracts are incomplete and quality is hard to specify or enforce, those same incentives can lead firms to reduce costs in ways that harm service quality (Hart et al. 1997). Healthcare is a prime example of this trade-off, and empirical evidence bears this out, with studies comparing public and private providers often documenting tensions between cost containment and quality of care (Knutsson and Tyrefors 2022, Chan et al. 2023, Duggan et al. 2023).
But what if private management could be introduced without the profit incentives that drive these trade-offs? Brazil offers a test case. Our research (Coube, Fontes, and Rocha 2026) investigates the country’s Organizações Sociais de Saúde (OSS) model, which has transferred the management of public hospitals to private non-profit organisations, while retaining public ownership of assets and governmental control over surplus rights. Hospitals remain publicly funded, with contracts linking payment to performance targets. They do not charge fees, do not compete for patients, and remain universally accessible. Managers bring private sector expertise and operate under private labour law, which grants considerably more flexibility over hiring, contracts, and procurement than public administration rules.
Studying the impact of outsourcing in Brazil’s public hospitals
We estimate the effects of the OSS model using a difference-in-differences approach. We compare public hospitals that switched to OSS management with similar public hospitals that remained under direct government administration, exploiting the fact that transitions occurred at different times across the country. To make the comparison credible, we match treated and control hospitals on key baseline characteristics and show that their outcomes followed similar trends prior to the transition. Our dataset covers the universe of hospitalisations in Brazil from 2006 to 2022, with detailed information on patient characteristics, length of stay, and discharge outcomes. We complement this with data on hospital inputs and administrative records covering the universe of Brazilian physicians, allowing us to track changes in hiring and separations, workforce composition, individual productivity, and employment contracts in unprecedented detail.
Sharp gains in production and efficiency, with no loss in quality
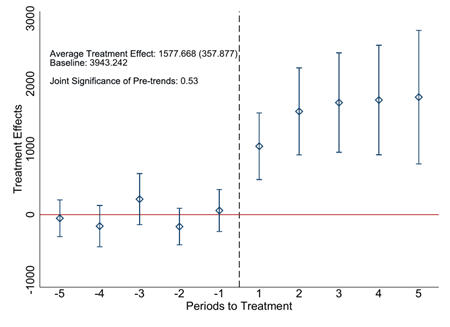
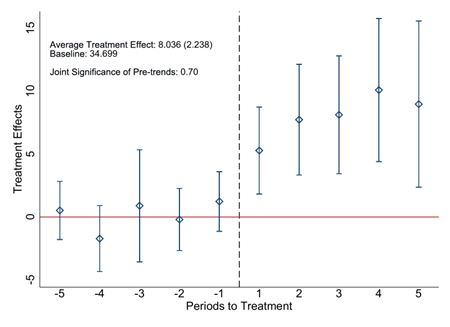
Following the transition to OSS management, hospital admissions increased by almost 40% relative to the baseline period (Figure 1A). This increase was broad-based, spanning surgical, clinical, obstetric, and emergency care. Hospitals also became substantially more efficient. Bed turnover rose by 23% (Figure 1B), bed occupancy increased by 14%, and risk-adjusted length of stay fell by 8%. These productivity gains are comparable in magnitude to those documented in studies of competition-enhancing policies and management interventions (e.g. Bloom et al. 2015, Gaynor et al. 2013, Muñoz and Otero 2025).
An important question is whether these gains came at the expense of care quality. We find no evidence that they did. Risk-adjusted inpatient mortality (Figure 1C) and readmission rates remained unchanged following the transition to OSS management. This holds across different patient groups, including those with the most severe conditions. We also find no change in the risk composition of patients, which rules out the possibility that OSS hospitals improved performance by selectively admitting easier cases. Nor do we detect shifts in observable patient characteristics such as age, gender, or income, easing concerns that the gains came at the expense of equity.
Figure 1: Effects on hospital production, productivity, and quality
Panel A: Hospital admissions
Panel B: Bed turnover
Panel C: Risk-adjusted patient mortality
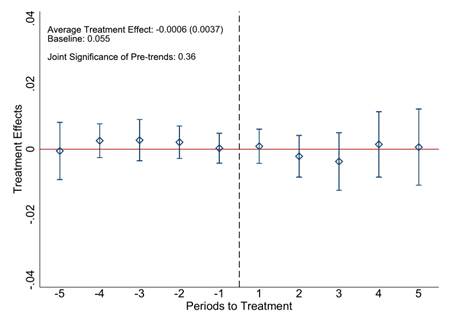
Note: This figure plots the pre- and post-treatment effects of the OSS model on hospital admissions (panel A), bed turnover rates (panel B), and risk-adjusted inpatient mortality (panel C). The Average Treatment Effect is computed as the average of the post-treatment estimates. The baseline corresponds to the sample mean for treated hospitals in the five years prior to OSS adoption. The figure also reports the p-value from an F-test of the joint significance of the pre-treatment coefficients.
More hospital care, better access, lower mortality
Did the additional hospital output actually benefit patients, or did it simply reflect overuse? We extend the analysis to the municipal level and find that the rise in hospital admissions translated largely into expanded hospital access for the local population. The effects were strongest in municipalities with the greatest initial scarcity of hospital beds, where admissions rose by 33%. Population mortality declined, falling by 3% on average. The reduction was concentrated in deaths occurring outside health facilities (at home or in public spaces), suggesting that OSS hospitals reached individuals who might otherwise have died without accessing care. In municipalities with the lowest initial bed supply, mortality fell by 6.4%.
How private managers transformed hospital operations
A distinctive feature of our research is that we can trace the channels behind the performance gains, opening the black box of what private managers actually did differently inside public hospitals. The gains did not come primarily from expanding physical capacity. Bed capacity expanded modestly (by about 14%), accounting for only about a third of the increase in output. There were no major investments in advanced medical equipment. Instead, most of the improvement came from using existing resources more efficiently.
The biggest changes occurred in personnel management. OSS managers reshaped the physician workforce in important ways. They moved away from rigid public-sector employment arrangements and towards more flexible contracts. The share of physicians under civil-service-style contracts fell by 24 percentage points, while the share working under independent contracts, where pay can be more closely tied to output, rose by 17 percentage points. They also increased the share of physicians with formal specialty titles by 13%, indicating a marked shift towards a more qualified workforce. And they used their hiring flexibility actively: the share of newly hired physicians jumped by 30% in the first year after the transition, with new recruitment tilted towards more qualified doctors hired under more flexible contracts.
Just as importantly, using physician-level data, we find that separation rates among incumbent doctors rose sharply after the transition to OSS. But these exits were not random. They were heavily concentrated among physicians in the bottom quartile of the baseline productivity distribution, measured by the number of inpatient cases handled per hour worked (Figure 2). Exit rates for this group rose by 15 percentage points, while the most productive doctors were largely retained. In parallel, output per physician increased by 24% on average. This suggests that OSS gains reflected not only greater managerial flexibility, but the deliberate use of that flexibility to build a more productive medical workforce.
Figure 2: Effects on incumbent physician separations by baseline productivity
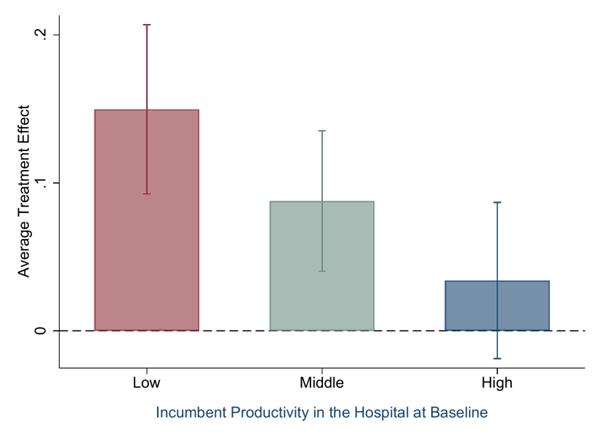
Note: This figure plots the average effects of the OSS model five years after the treatment on the separation rate of incumbent physicians, shown separately for incumbents with low (first quartile), medium (second and third quartiles), and high (fourth quartile) baseline productivity. Productivity is measured as the number of cases handled per hour worked by each incumbent physician at baseline.
The importance of managerial capacity
Expanded managerial discretion did not automatically translate into better performance. When we compare hospitals managed by more- and less-experienced OSS organisations, the differences are stark. Hospitals run by more experienced firms saw admissions rise by 54% and bed turnover increase by 40%, while those managed by less experienced firms achieved gains of only 21% and 3%, respectively (Figure 3). More experienced firms were also much more likely to implement the efficiency-oriented personnel practices described above. They made greater use of flexible employment contracts, hired more aggressively, and separated a larger share of low-productivity physicians. Less experienced firms, by contrast, relied mainly on expanding bed capacity, a costlier and less efficient route to higher output.
This pattern is not unique to firm experience. It also appears when we use other measures of managerial capacity, including managers’ industry-specific experience, permanent earnings capacity, and broader organisational quality indices. Across the board, higher-capacity organisations generated larger productivity gains and greater reductions in population mortality. These results suggest that relaxing public-sector constraints is insufficient to improve performance. Flexibility yields the greatest gains when placed in the hands of managers who can translate autonomy into more efficient organisational and personnel practices.
Figure 3: Effects on hospital output and productivity by OSS organisational experience
Panel A: Hospital admissions
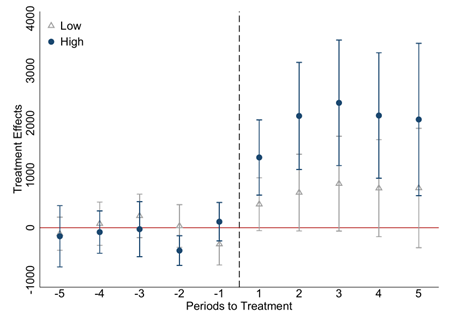
Panel B: Bed turnover
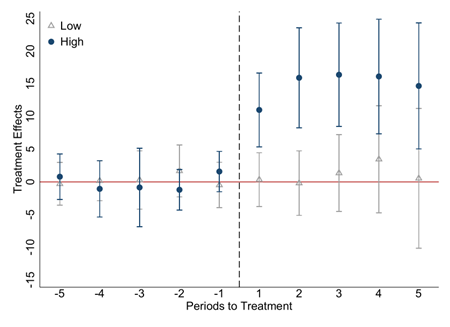
Note: This figure plots the treatment effects of the OSS model on hospital admissions (panel A) and bed turnover rates (panel B), separately by whether the hospital is managed by a firm with above-median (High) or below-median (Low) experience.
Policy implications
Our findings offer important lessons for governments considering outsourcing in complex public services, particularly in settings where contracts are incomplete and quality is difficult to measure or enforce. The OSS experience suggests that hybrid governance arrangements, transferring management to private operators while preserving public ownership, public funding, and limits on profit extraction, can deliver efficiency gains without sacrificing quality or equity.
But greater managerial flexibility alone is not enough. Recent research shows that the quality of managers and bureaucrats matters for public-sector performance even within the rigid boundaries of public administration (Fenizia 2022, Best et al. 2023, Muñoz and Otero 2025). We further show that even outside these boundaries, after relaxing public-sector constraints and expanding managerial autonomy, improvements still depend on the quality of managers: the benefits of expanded discretion within government organisations materialise primarily when it is paired with managers who are capable of translating autonomy into efficient organisational practices. For policymakers, this means that provider selection is central to realising the full potential of outsourcing. Our results therefore reinforce the view that managerial capacity remains a central determinant of performance in public service delivery, both within and beyond the constraints of public-sector institutions.
These insights may extend well beyond Brazil. Public administrations in many countries face similar underlying challenges, including rigid administrative rules, limited managerial autonomy, and weak accountability for performance. As a result, many have pursued outsourcing reforms, generating substantial variation in how these arrangements are designed across and within public sectors. This variation in design and in who is selected to run these arrangements may go a long way towards explaining why some reforms succeed while others do not.
References
Best, M C, J Hjort, and D Szakonyi (2023), "Individuals and organizations as sources of state effectiveness," American Economic Review, 113(8): 2121–2167.
Bloom, N, C Propper, S Seiler, and J Van Reenen (2015), "The impact of competition on management quality: Evidence from public hospitals," Review of Economic Studies, 82(2): 457–489.
Chan, D C, D Card, and L Taylor (2023), "Is there a VA advantage? Evidence from dually eligible veterans," American Economic Review, 113(11): 3003–3043.
Coube, M, L F Fontes, and R Rocha (2026), "Public services under private management," Unpublished manuscript.
Duggan, M, A Gupta, E Jackson, and Z S Templeton (2023), "The impact of privatization: Evidence from the hospital sector," Unpublished manuscript.
Fenizia, A (2022), "Managers and productivity in the public sector," Econometrica, 90(3): 1063–1084.
Gaynor, M, R Moreno-Serra, and C Propper (2013), "Death by market power: Reform, competition, and patient outcomes in the National Health Service," American Economic Journal: Economic Policy, 5(4): 134–166.
Hart, O, and J Moore (1990), "Property rights and the nature of the firm," Journal of Political Economy, 98(6): 1119–1158.
Hart, O, A Shleifer, and R W Vishny (1997), "The proper scope of government: Theory and an application to prisons," Quarterly Journal of Economics, 112(4): 1127–1161.
Knutsson, D, and B Tyrefors (2022), "The quality and efficiency of public and private firms: Evidence from ambulance services," Quarterly Journal of Economics, 137(4): 2213–2262.
Muñoz, P, and C Otero (2025), "Managers and public hospital performance," American Economic Review, 115(11): 4040–4074.