

Child stunting was eradicated in developed countries during the 19th and 20th centuries. These cases yield lessons for combating stunting today.
Child malnutrition is one of the most pressing and persistent global health challenges in the world today. The leading indicator of child malnutrition is the stunting rate, which is the percentage of children under the age of 5 who are short for their age relative to modern growth standards. While there has been a reduction in child stunting rates from 40% in 1990 to 23% in 2016, 155 million children worldwide still suffer from stunted growth, mostly in Africa, South Asia, and Southeast Asia (see Figure 1). Reducing child stunting is therefore a target under the Sustainable Development Goals. Stunting matters not only because it causes the children experiencing it misery, but also because it has long-run consequences for these children later in their life. Stunted children have worse outcomes across a range of indicators: they perform poorly on cognitive tests, receive fewer years of schooling, have lower incomes as adults, and are more likely to live in poverty (Hoddinott et al. 2013). Reducing stunting can increase the capabilities and welfare of a population many years into the future.
Figure 1 Map of stunting prevalence around the world in 2015

What causes child stunting?
The causes of child stunting are multidimensional, ranging from inadequate nutrition to repeated disease insults. A poor diet lacking in calories, protein or other micronutrients at early ages clearly matters. Mounting evidence also suggests that sources of animal protein in the diet may be particularly important in preventing children from growing too slowly (Headey et al. 2017). Hygiene practices and sanitation infrastructure are also important, especially access to piped water in the home, hand washing and access to toilet facilities (Nabwhera et al. 2017). Spears et al. (2013) and Lin et al. (2013) find that the prevalence of open defecation strongly influences stunting by exposing children to pathogens that lead to chronic diarrhoea and malabsorption of the nutrients they consume.
In September 2017, academics from a broad range of disciplines, policy experts and influencers in the third sector, and international organisations met at the LSE to discuss the current state of stunting research and policy at a conference entitled ‘Stunting: Past, Present, Future’ (Schneider 2018). Importantly, many economic historians attended the conference providing a long-run perspective on child stunting. This column highlights a few key lessons for stunting research that come from taking a long-run, historical view on the issue.
Evidence from stunting research
- The first lesson is that stunting is not solely a modern phenomenon. Analysing a number of historical sources for children under 5 or just above, it is clear that stunting was probably as prevalent in developed countries in the early 20thcentury as it is in developing countries today (see Figure 2). The best historical data are drawn from Japan and the US. Japan had stunting rates above 60% in the early 20thcentury, and although there was some improvement before World War II, only after the war did the stunting rate decline rapidly to a very low level. In the US stunting was always less prevalent, with only 17% of children stunted in 1918; although adults were especially tall in the US in the late nineteenth century compared to other populations, so some of the decrease in stunting had already occurred (NCD Risk Factor Collaboration 2016).
Figure 2 Stunting rates around the world through the 20th century
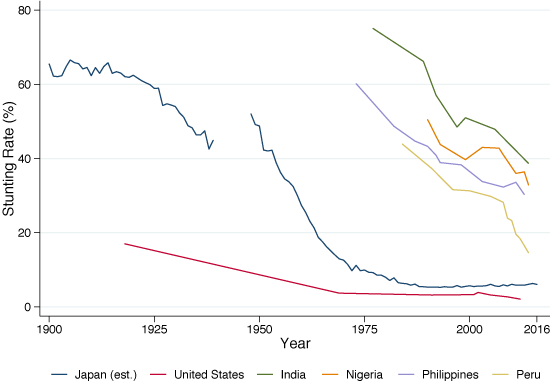
Sources: US – Roberts (2018) and World Bank Data Bank; Japan – Schneider and Ogasawara (2018); Others – World Bank Data Bank.
- The reduction in the prevalence of stunting is best understood as part of the increase in adult height and the change in the growth pattern of children observed over the past 150 years in most countries (Cole and Mori 2017). The sharp decline in the stunting rate in Japan was the mirror image of the 14.6-16cm increase in mean adult height, and a reduction of around two years in the average age of the pubertal growth spurt. This secular increase in height occurred across the world to a greater or lesser extent for both men and women (see Figure 3). The historical literature has tended to emphasise reductions in child morbidity through better sanitation infrastructure and hygiene practices (Hatton 2014), and improvements in nutrition – particularly milk consumption – as being important for improving adult stature (Baten and Blum 2014). Thus, historical studies of the secular increase in height can reveal the types of changes in economic conditions that might lead to reductions in the stunting rate today.
Figure 3 Change in mean adult stature between the 1896 and 1996 birth cohorts
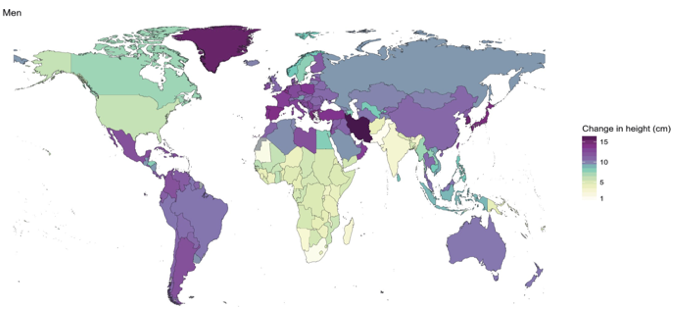
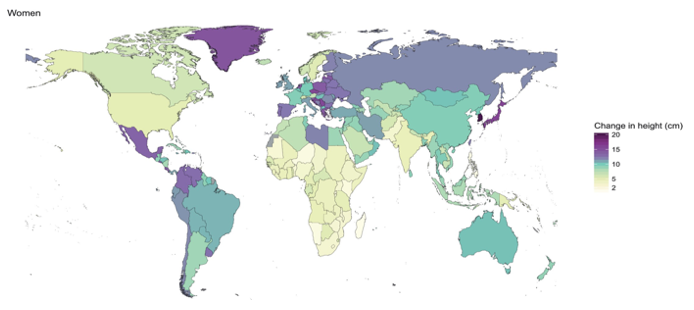
Sources: NCD Risk Factor Collaboration (2016).
- Figure 2 highlights that reducing stunting is a long-run process which takes decades. Japan eradicated stunting on a national scale between 1948 and 1986 with the prevalence of stunting falling from 50% to 5.7% over that 40-year period. During that same period, life expectancy at birth increased 21.3 years and GDP per capita increased at an average annual rate of 5.8%. If it took nearly 40 years to eliminate stunting with rather favourable economic and public health conditions, then we must be realistic about the amount of time and policies required to eradicate child stunting in developing countries today.
- A final lesson from the conference, supported by a historical approach, is that we need more research on catch-up growth in adolescenceand its consequences for later outcomes. The traditional 1,000-days narrative suggests that stunted children are unable to make up for their slow growth in early childhood at later ages (Victora et al. 2010); however, many scholars including economic historians, nutritionists, and epidemiologists have noted that it is possible for children to experience catch-up growth between early childhood and adulthood. Steckel (1987) observed very large levels of catch-up growth between ages five and adulthood among slaves in the US South (Schneider 2017). In addition, Prentice et al. (2013) show that modern children also experience catch-up growth between early childhood and adulthood. Thus, it is important to explore whether adolescence could potentially be a critical period for interventions because there are many children who are already stunted. If it is possible to help these children with targeted interventions in adolescence, then we may be able to mitigate some of the long-run consequences of stunting on stunted children over the age of five, potentially improving their life-long health and earnings potential.
Clearly, understanding the history of child stunting reveals a number of useful lessons that can help combat stunting today. Eradicating stunting is a long-run process linked to changes in child growth and adult stature. It can take decades even in favourable economic and health conditions and seems to be driven by reductions in child morbidity and improvements in nutrition quality.
Author’s note: To read the full (including non-historical) findings of conference, please see the conference report (Schneider 2018) available here.
References
Baten, J and M Blum (2014), “Why are you tall while others are short? Agricultural production and other proximate determinants of global heights”, European Review of Economic History 18(2), 144–165.
Cole, T J and H Mori (2017), “Fifty years of child height and weight in Japan and South Korea: Contrasting secular trend patterns analyzed by SITAR”, American Journal of Human Biology 12, e23054–13.
Hatton, T J (2014), “How have Europeans grown so tall?”, Oxford Economic Papers 66(2), 349–372.
Headey, D D, K Hirvonen and J F Hoddinott (2017), “Animal sourced foods and child stunting”, IFPRI Discussion Paper, 50.
Hoddinott, J, J R Behrman, J A Maluccio, P Melgar, A R Quisumbing, M Ramirez-Zea, A D Stein, K M Yount and R Martorell (2013), “Adult consequences of growth failure in early childhood”, American Journal of Clinical Nutrition 98(5), 1170–1178.
Lin, A, B F Arnold, S Afreen, R Goto, T M N Huda, R Haque, R Raqib, L Unicomb, T Ahmed, J M Colford Jr and S P Luby (2013), “Household environmental conditions are associated with enteropathy and impaired growth in rural Bangladesh”, The American Journal of Tropical Medicine and Hygiene 89(1), 130–137. .
Nabwera, H M, A J Fulford, S E Moore and A M Prentice (2017), “Growth faltering in rural Gambian children after four decades of interventions: A retrospective cohort study”, The Lancet Global Health 5(2), e208–16.
NCD Risk Factor Collaboration (2016), “A century of trends in adult human height”, eLife, 1–29.
Prentice, A M, A K Ward, G R Goldberg, L M Jarjou, S E Moore, A J Fulford and A Prentice (2013), “Critical windows for nutritional interventions against stunting”, American Journal of Clinical Nutrition 97(5), 911–918.
Schneider, E B (2017), “Children's growth in an adaptive framework: Explaining the growth patterns of American slaves and other historical populations”, The Economic History Review 70(1), 3–29..
Schneider, E B (2018), Stunting: past, present, future, Conference Report, Department of Economic History, London School of Economics and Political Science, London, UK.
Spears, D, A Ghosh and O Cumming (2013), “Open defecation and childhood stunting in India: An ecological analysis of new data from 112 districts”,PLoS ONE, 8(9), e73784–9. http://doi.org/10.1371/journal.pone.0073784.
Steckel, R H R (1987), “Growth depression and recovery: The remarkable case of American slaves”, Annals of Human Biology 14(2), 111–132.
Victora, C G, M de Onis, P C Hallal, M Blossner and R Shrimpton (2010), “Worldwide timing of growth faltering: Revisiting implications for interventions”, Pediatrics, 125(3), e473–e480.