







In Rwanda, telemedicine delivered higher-quality, faster, and lower-cost care for common conditions.
Mobile technologies have enabled low-cost, accessible scaling of services in finance, labour markets, and healthcare. Telemedicine, in particular, has expanded access to care (Hollander and Carr 2020, Dahlstrand 2021, Goetz 2023, Uscher-Pines and Mehrotra 2014), but critics have raised concerns about the quality of virtual care, for example, due to the lack of physical exams or changes in patient-provider communication (Miller 2003, Henry et al. 2017, Alpert 2024). This is especially important given the recent rise in the use of telemedicine and patients’ use of virtual care as a substitute for traditional in-person services (Ashwood et al. 2017, Shah et al. 2018, Ellegård et al. 2021, Rabideau and Eisenberg 2022).
Despite the high stakes in medical care settings, little is known about how care delivered in a virtual visit differs from the care delivered in a traditional face-to-face visit (Henry et al. 2017, Miller 2003, Lagarde et al. 2024). In recent work (Wellsjo et al. 2025), we help fill this gap by analysing the differences in care between telemedicine and in-person care at scale in Rwanda. We consider both (1) quality of care or correct case management in terms of the use of appropriate diagnostic tests and prescribed medications, as well as the evaluation of symptoms and medical history, and (2) cost of care in terms of unnecessary tests and medications, as well as time and monetary costs.
A key challenge is that patients who choose to receive care virtually through telemedicine are likely different from those who seek care face-to-face (Fadlon et al. 2024, Lagarde et al. 2024, Shah et al. 2018). We overcome this challenge by using an audit study with standardised patients (SPs) to compare the quality and cost of virtual and in-person care. SPs are locally recruited individuals who are trained to present a standardised case scenario as real patients to providers, both in person and remotely. The SP method is considered the gold standard approach to make apples-to-apples comparisons across visits (Peabody et al. 2000, Kwan et al. 2019).
Comparing the quality and efficiency of telemedicine and in-person care in Rwanda
We study these questions in Rwanda, where Babyl, a nationwide telemedicine platform, provides phone-based clinical consultations and a text-based system for digital prescriptions and lab orders that can be filled at participating health facilities and pharmacies. Launched in partnership with the Rwandan government, Babyl has achieved widespread adoption with more than 2.5 million registered users (18% of the population). This offers a unique opportunity to evaluate telemedicine as a large-scale alternative to in-person care.
We focus on two important diseases that are high incidence and can be treated remotely via telemedicine: acute malaria and upper respiratory infection (URI). These illnesses rank among the top five diagnoses treated in the telemedicine platform. We selected these cases not only for their relevance but also because they allow us to compare how the medium affects care in low- and high- discretion cases. Malaria has a clear and effective recommended protocol. URI symptoms, such as a cough and sore throat, are non-specific which makes diagnosis challenging and introduces room for provider discretion in treatment.
Telemedicine is higher quality and more efficient than in-person care
In this study, we used the SP method to present the same clinical case scenarios by ‘real’ patients for malaria and URI in both virtual and in-person care settings. Our main analysis compares the SP outcomes of interest between virtual and in-person settings, summarised in Figure 1.
Quality of care outcomes in telemedicine (compared to in-person care):
- Although SPs presenting malaria symptoms remotely were just as likely to receive correct case management, SPs presenting URI symptoms were roughly 200% more likely to be correctly managed.
- Providers asked SPs more questions about symptoms and medical history (60% and 100% more for malaria and URI, respectively).
- Providers prescribed almost 15% more optional medicines, not essential, but helpful to alleviate patients’ symptoms.
Efficiency outcomes in telemedicine (compared to in-person care):
- Providers gathered more information and provided the same or better care during consultations that were around 30% shorter.
- SPs also received care faster, waiting more than an hour less for a consultation.
- Providers prescribed fewer unnecessary drugs (almost 15% and 40% fewer for malaria and URI, respectively) and ordered around 70% fewer unnecessary labs.
- SPs paid approximately 20% less out-of-pocket for malaria visits and 40% less for URI visits.
Figure 1: Differences between telemedicine and in-person care
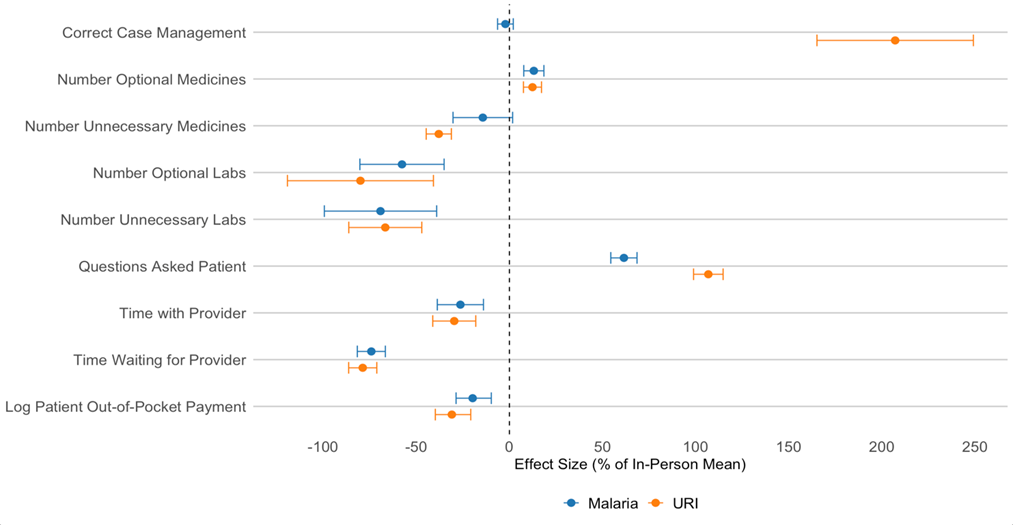
Notes: Estimated SP outcomes in telemedicine as a percentage change from the average value for in-person visits. Figure plots the point estimate and 95% confidence intervals.
Are differences driven by the types of providers who work in telemedicine?
An important policy question is whether telemedicine is better because the providers who work there are higher quality, or because the medium changes medical decision-making. If this is due to better providers working via telemedicine, the high quality of telemedicine may not continue to scale if the platform were further expanded to include lower quality providers. There are differences between in-person and telemedicine providers and their work setting that may explain the results. Telemedicine providers have more training and medical knowledge than those who provide care in person at health facilities. Providers who consult on the telemedicine platform typically do so part-time and report being significantly less overwhelmed, feeling less rushed, and less emotionally exhausted than their in-person peers. However, none of these differences in provider characteristics or reported effects of the work environment explain our results. The differences in quality and cost outcomes between remote and in-person care remain even after controlling for these characteristics.
What explains the superior outcomes in telemedicine?
Remote encounters over the phone seem to improve provider-patient communication compared to face-to-face encounters. We surveyed a subset of telemedicine providers who also saw patients in person about their experiences in virtual versus face-to-face visits, summarised in Figure 2.Providers reported that remote communication makes it easier to get information and relate to patients, perhaps due to a reduction in distractions when consulting in a quiet call centre relative to in-person clinic care, which can be busy and loud. Providers also reported that remote consultations are less tiring and shorter. SP assessments of their visits match this description; SPs reported clearer communication, more language they could understand, a better explanation of their illness, and that it was easier for the SP to convey their symptoms over the phone. During in-person visits, SPs were more likely to report that the provider appeared distracted and that there was background noise during the consultation.
Figure 2: Provider ratings of phone vs. in-person care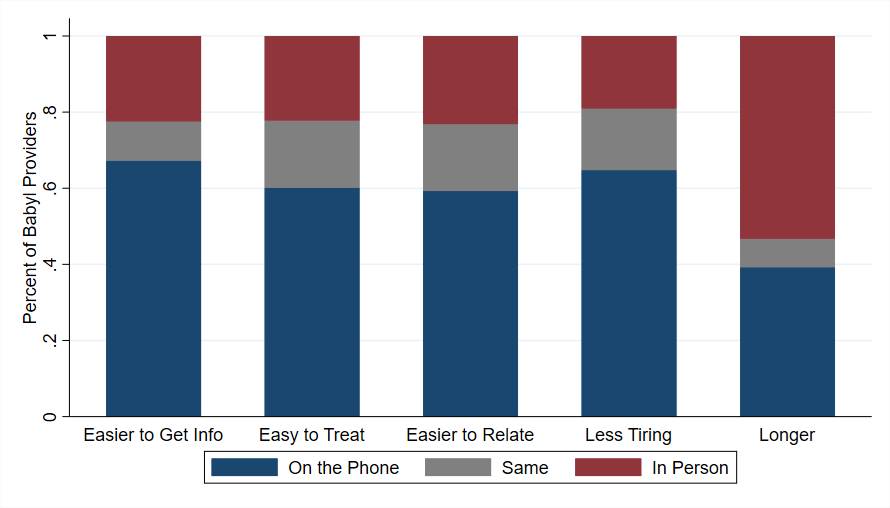
Notes: Figure summarises provider perceptions of patient care in person versus over the phone as measured in the provider survey. Provider ratings of how easy it is to get information from, treat, and relate to patients were selected from the options: a lot easier on the phone, a little easier on the phone, the same on the phone and in person, a little easier in person, a lot easier in person. Figure also summarises providers’ responses to questions about how tiring their interactions were (options ranging from a lot more tiring on the phone to a lot more tiring in person) and about the length of their interactions (options ranging from a lot longer on the phone to a lot longer in person). For the figure, we collapse the five categories into three: a lot and a little more on the phone, the same, and a lot and a little more in person.
Patient requests for unnecessary antibiotics
To further explore how telemedicine changes medical decision-making, we also tested how providers treat assertive patients who suggest a diagnosis or ask for a specific treatment. When SPs requested an unnecessary antibiotic, providers in face-to-face interactions were significantly more likely to give it to the SP than if the SP did not make the request (18pp and 7pp more likely for malaria and URI, respectively). However, this was not the case in virtual visits, where providers were no more likely to prescribe an unnecessary antibiotic than instances where the SP did not make the request. This was not because providers weren’t listening in virtual visits. When SPs suggested a COVID-19 diagnosis, they were 25pp more likely to be ordered a COVID-19 test, regardless of whether the visit was conducted in-person or virtually. Rather, providers in our survey reported that that they feel less pressure to agree to patient requests over the phone.
Implications for health policy
Our research has several policy implications for the use and expansion of telemedicine.
- Use of telemedicine: At least for the common conditions studied in our setting, telemedicine outperforms traditional in-person care settings. An expansion of telemedicine services can provide high-quality, efficient care.
- Overprescribing: Moving from in-person to virtual visits may help to reduce overprescribing of antibiotics, especially in response to patient requests.
- Work environment: The less distracting work environment in telemedicine appears to play a key role in improving patient-provider communication. When thinking about what features are key for the success of a telemedicine platform, replicating the quiet consultation call centre may be a central piece.
More work comparing telemedicine to in-person care will help us to understand how much these results generalise to other settings and conditions, such as those that are more serious or require ongoing care.
References
Alpert, J S (2024), “Face-to-face versus digital encounters in the clinic,” American Journal of Medicine 137(5): 379–380.
Ashwood, J S, A Mehrotra, D Cowling, and L Uscher-Pines (2017), “Direct-to-consumer telehealth may increase access to care but does not decrease spending,” Health Affairs 36(3): 485–491.
Dahlstrand, A (2021), “Defying distance? The provision of services in the digital age,” Unpublished manuscript.
Ellegård, L M, G Kjellsson, and L Mattisson (2021), “An app call a day keeps the patient away? Substitution of online and in-person doctor consultations among young adults,” Unpublished manuscript.
Fadlon, I, P Agnihotri, C Longhurst, and M Tai-Seale (2024), “Equity and efficiency in technology adoption: Evidence from digital health,” Unpublished manuscript.
Goetz, D (2023), “Telemedicine competition, pricing, and technology adoption: Evidence from talk therapists,” International Journal of Industrial Organization 89: 102956.
Henry, B W, D E Block, J R Ciesla, B A McGowan, and J A Vozenilek (2017), “Clinician behaviors in telehealth care delivery: A systematic review,” Advances in Health Sciences Education 22: 869–888.
Hollander, J E, and B G Carr (2020), “Virtually perfect? Telemedicine for COVID-19,” New England Journal of Medicine 382(18): 1679–1681.
Kwan, A, B Daniels, S Bergkvist, V Das, M Pai, and J Das (2019), “Use of standardised patients for healthcare quality research in low- and middle-income countries,” BMJ Global Health 4(5): e001669.
Lagarde, M, I Papanicolas, and N Stacey (2024), “The demand for private telehealth services in low- and middle-income countries: Evidence from South Africa,” Social Science & Medicine 116570.
Miller, E A (2003), “The technical and interpersonal aspects of telemedicine: Effects on doctor–patient communication,” Journal of Telemedicine and Telecare 9(1): 1–7.
Peabody, J W, J Luck, P Glassman, T R Dresselhaus, and M Lee (2000), “Comparison of vignettes, standardized patients, and chart abstraction: A prospective validation study of three methods for measuring quality,” Journal of the American Medical Association 283(13): 1715–1722.
Rabideau, B, and M Eisenberg (2022), “The effects of telemedicine on the treatment of mental illness: Evidence from changes in health plan benefits,” Unpublished manuscript.
Shah, S J, L H Schwamm, A B Cohen, M R Simoni, J Estrada, M Matiello, A Venkataramani, and S K Rao (2018), “Virtual visits partially replaced in-person visits in an ACO-based medical specialty practice,” Health Affairs 37(12): 2045–2051.
Uscher-Pines, L, and A Mehrotra (2014), “Analysis of Teladoc use seems to indicate expanded access to care for patients without prior connection to a provider,” Health Affairs 33(2): 258–264.
Wellsjo, A S, P Gertler, A Kwan, E Remera, P Irakiza, J Condo, and J Humuza (2025), “The medium matters: Medical decision-making in telemedicine versus in-person care,” Unpublished manuscript.