


Research on Ghana found that providing low-income adults with small, regular mobile communication credits significantly reduced mental distress and domestic violence during COVID-19.
Nearly one billion people globally suffer from mental health disorders (Lancet Global Health 2020). The COVID-19 pandemic resulted in a 25% increase in the global prevalence of mental disorders, particularly anxiety and depression, in the first year alone (WHO 2022). This may have been due to higher levels of stress caused by social isolation during the pandemic, as well as limits on individuals’ ability to work and seek support from loved ones.
Recent research has highlighted that these negative effects on mental health were particularly severe for certain groups, with young people and women experiencing disproportionately worse mental health outcomes (Xiong et al. 2020). Paradoxically, policies implemented by governments to reduce the spread of the disease, such as lockdowns and social distancing, also had the unintended effect of increasing levels of stress and social isolation.
Given that climate change is expected to increase the frequency of epidemics in the future, investigating which policy interventions can help improve mental health is of crucial importance to improve overall health and human capital (Archibong and Annan 2023, Carleton and Hsiang 2016). This is especially true given the potentially large economic losses incurred by mental health disorders. For instance, the two most common mental disorders – anxiety and depression – are estimated to cost the global economy approximately US$1 trillion each year, with total costs projected to rise to $6 trillion by 2030 (Lancet Global Health 2020).
A communication intervention to improve mental health outcomes
In forthcoming research, we answer this question using evidence from a communication intervention in Ghana (Annan and Archibong 2023, Annan and Archibong 2022). We investigate whether improving individuals’ ability to communicate with each other, using information and communication technology such as mobile phones, can improve mental health. Partnering with a major telecommunications company, we implemented low-cost communication interventions that provided mobile calling credits to a nationally representative set of low-income adults in Ghana during COVID-19. We find that individuals’ ability to make unexpected calls or seek digital loans increased significantly, while their need to borrow SOS airtime also decreased significantly relative to the control group. As a result, the programmes led to a significant decrease in mental distress (-9.8%) and lowered the likelihood of severe mental distress by 2.3 percentage points (a quarter of the mean prevalence).
The effects were stronger, larger, and more sustained among individuals provided a repeated instalment of monthly mobile credits rather than a single lump sum. The instalment communication credit programme also led to a significant decrease in domestic violence; specifically, a decline in the overall likelihood of individuals threatening their partners. The results also show that these effects were only through a reduction in mental distress, and that there was no impact on consumption spending.
Simple cost-benefit analysis shows that providing communication credit to low-income adults is a cost-effective policy for improving mental health, with each $1 of spending on communication credit delivering more than $1 in benefits to its beneficiaries. This demonstrates that communication – the ability to stay connected – meaningfully improves mental well-being and that such interventions are particularly valuable when implemented through numerous instalments.
Why and how might communication improve mental health and wellbeing?
Conceptually, communication is a network good, or a good whose value increases the more people use it. As a network good, it could improve mental health through at least three channels:
- Business-related services (via professional networks): Professional networks operate in the form of affected individuals being able to stay in touch with customers and buy/sell with vendors to increase their revenues, which has a positive impact on mental well-being (Ridley et al. 2020).
- Social inclusion and/or protection (via social networks): Social inclusion (or reduced isolation) operates in the form of individuals being able to stay in touch with friends/family who can provide emotional support (Mullainathan and Shafir 2013, Leslie and Wilson 2020), or serve as agents of social control and protection, reducing domestic violence by increasing the cost of violence (Gelles and Straus 1979).
- Informal insurance arrangements or consumption insurance (via social networks): In vulnerable periods such as COVID-19 related lockdowns, households may have difficulty communicating with their informal insurance networks (family, friends, etc.), causing their consumption risk-sharing ability to suffer (Blumenstock et al. 2016, Jack and Suri 2016).
An experimental approach: Studying the impact of ICT on mental health
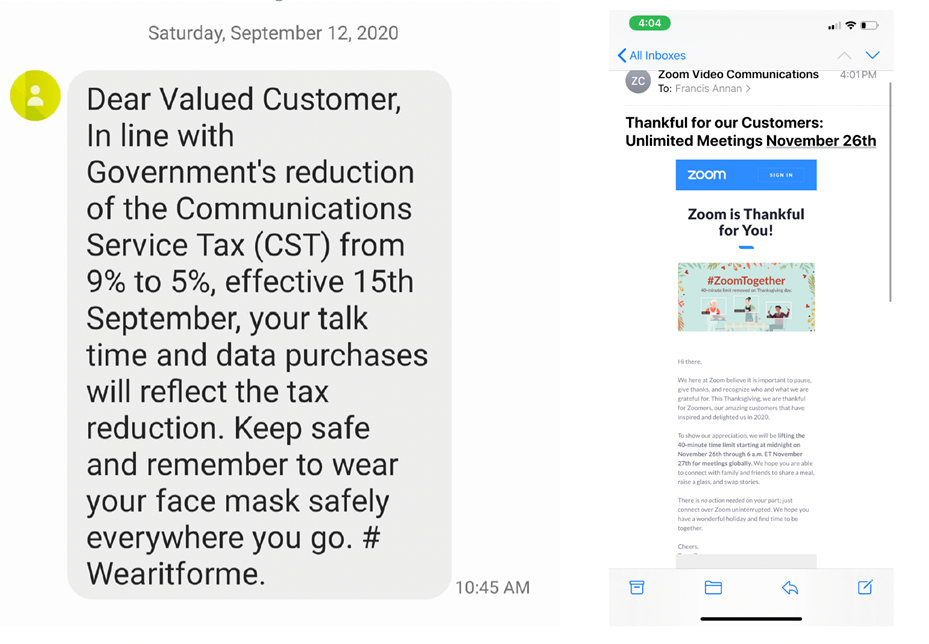
Around the world, major communication interventions were initiated in response to the COVID-19 pandemic, both in the public and private sectors. In the US, ATT Inc. provided 10GB of free internet data per month for 60 days as temporary relief for eligible customers (ATT Inc. 2020). In Ghana, the government reduced the Communication Service Tax (CST) from 9% to 5% in response to economic hardship, reducing the cost of mobile talk time and data purchases (see Figure 1, Ghana Revenue Authority 2020). Such communication programmes were especially vital in developing countries with large informal sectors, where COVID-19 posed severe credit, savings, and psychological challenges. Despite the increase in these communication-based programmes, there is relatively little evidence on their impacts on well-being during the pandemic.
Figure 1: Communication programmes from the Ghanaian government (left) and Zoom (right)
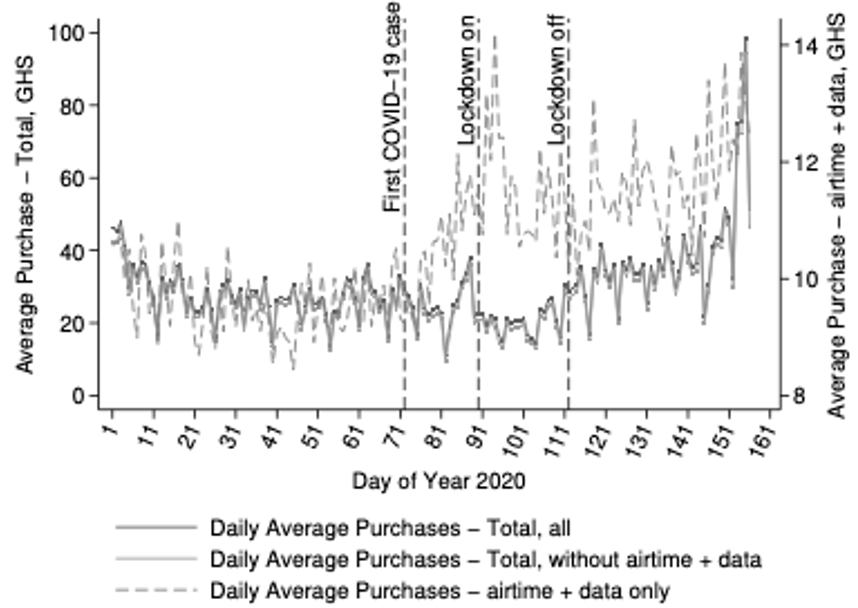
Using administrative data on mobile financial transactions from a major provider in Ghana in 2020, we estimate the potential value of communication during the pandemic. Examining this data reveals a striking difference in the patterns of overall market activity versus demand for mobile airtime related activities (as measured by the purchase of data and airtime amounts) among consumers following the onset of the pandemic and introduction of lockdown measures in March 2020. Figure 2 shows that while overall market activity decreased, demand for mobile airtime-related activities notably increased over the period. We conducted an RCT to estimate the effects of a short-term ‘mobile phone calling credit’ among a nationally representative set of low-income households.
Figure 2: Decrease in overall market activity but increased demand for mobile airtime/purchases in Ghana in 2020
We randomly assigned 1,131 individuals to two communication programmes: 40GHS ($7) lumpsum mobile credit versus 20GHS ($3.5) monthly instalments of mobile credit over two months, and then measured how this affected individuals’ ability to mitigate unexpected communication constraints.
Conceptually, programmes that facilitate communication during pandemics could be transformative, particularly for individuals facing other income constraints. Not having to worry about the ability to stay connected could free up the mental and emotional bandwidth necessary to burgeon through a pandemic and its constant uncertainty. Our interventions were designed to relax such constraints and evaluate their impact on mental health, domestic violence, and consumption expenditures.
Communication credit improved mental health, with instalment credit proving more effective
Three main results of the effects of the communication credits are detailed here:
- As a first stage, the interventions decreased unexpected communication constraints significantly. That is, our interventions enabled people to stay connected. These effects are larger and more sustained over time for the instalment communication credit programme compared to the lumpsum credit.
- We find meaningful improvement in psychological well-being, which is measured using the Kessler Psychological Distress Scale (K10). Mental distress decreased (-9.8%); severe mental distress decreased (-24%) relative to a control group. The instalment communication credit programme had larger, more sustainable effects compared to the lumpsum credit. Relatedly, only the instalment programme led to a significant decrease (-6.3%) in the overall likelihood of individuals threatening their partners.
- We find no improvement in direct economic well-being. There is no overall effect on total consumption, which is reassuring as the size and specificity of our intervention were not large enough to meaningfully change consumption.
Policy implications for ICT and mental health
Our results suggest that, during periods of unexpected shocks with severe consequences for wellbeing, policymakers can improve mental health by expanding ICT access via communication credits, enabling individuals to stay connected to social and professional networks. This is a cost-effective means to support mental health, especially in low-income settings with limited resources.
References
Annan, F, and B Archibong (2023), “The value of communication for mental health,” NBER Working Paper [conditionally accepted at The Economic Journal].
Annan, F, and B Archibong (2022), “How can information and communication technology be leveraged to improve mental health?,” Brookings.
Archibong, B, and F Annan (2023), “Climate change, epidemics, and inequality,” Review of Environmental Economics and Policy 17(2): 336–345.
Blumenstock, J, N Eagle, and M Fafchamps (2016), “Airtime transfers and mobile communications: Evidence in the aftermath of a natural disaster,” Journal of Development Economics 120(C): 157–181.
Carleton, T A, and S M Hsiang (2016), “Social and economic impacts of climate,” Science 353(6304): aad9837.
Gelles, R J, and M Straus (1979), “Determinants of violence in the family: Toward a theoretical integration,” Contemporary Theories about the Family.
Ghana Revenue Authority (2020), “Communication service tax.”
Jack, W, and T Suri (2016), “The long-run poverty and gender impacts of mobile money,” Science 354(6317): 1288–1292.
Lancet Global Health (2020), “Mental health matters,” The Lancet Global Health 8(11): e1352.
Leslie, E, and R Wilson (2020), “Sheltering in place and domestic violence: Evidence from calls for service during COVID-19,” Journal of Public Economics 189: 104241.
Mullainathan, S, and E Shafir (2013), “Scarcity: Why having too little means so much,” Time Books.
Ridley, M W, G Rao, F Schilbach, and V H Patel (2020), “Poverty, depression, and anxiety: Causal evidence and mechanisms,” Science 370(6522): 94–108.
World Health Organization (WHO) (2022), “COVID-19 pandemic triggers 25% increase in prevalence of anxiety and depression worldwide.”
Xiong, J, O Lipsitz, F Nasri, L M Lui, H Gill, L Phan, et al. (2020), “Impact of COVID-19 pandemic on mental health in the general population: A systematic review,” Journal of Affective Disorders 277: 55–64.