






Among women in rural Ghana, depression and anxiety reduce take-up for jobs outside the home, but have no effect on productivity or earnings when the same job is offered at home – suggesting that work environment is a key barrier to labour market participation.
Editor’s note: For a broader synthesis of themes covered in this article, check out Issue 2 of our VoxDevLit on Female Labour Force Participation.
Poor mental health is prevalent in low-income populations around the world and is associated with low labour supply and earnings, creating negative feedback loops that may perpetuate poverty (Ridley et al. 2020, WHO 2022, Hakulinen et al. 2019, Biasi et al. 2021, Mojtabai et al. 2015, Lund et al. 2024, de Quidt and Haushofer 2016, Barker et al. 2022). In line with global patterns, we find that, among poor women in rural Ghana, 39.7% were suffering from depression and 45% were experiencing anxiety.
Decomposing the relationship between labour market outcomes and mental health
Relatively little is known about the channels through which poor mental health reduces labour participation and income – or whether it is driven by low job take-up, poor performance on the job, or higher quit rates. To better understand how mental health conditions relate to these important outcomes, we examine the relationship between mental health and labour market outcomes. Specifically, we conduct a two-phase study to decompose how depression and anxiety relate to (i) job take-up decisions, (ii) labour supply, output, and earning conditional on job take-up, and (iii) quit rates (Carvalho, de Walque, Lund, Schofield, Somville, and Wei 2026).
Phase 1: Job offers outside versus inside the home
In the first phase of our study, to avoid selection due to search or endogenous job offers, we make attractive and identical job offers to participating women. The work offered involves stitching bags, which is similar to cash-for-work opportunities often provided by governments with the aim of supporting the poor during the lean season: it is part-time, low-skill, and offers a wage premium of roughly 50%. Further, the decision to work is high stakes, with the income provided by the job accounting for about 46% of average total household income during this period. We elicit willingness to work under two different scenarios: work from home or work from a common nearby worksite. This variation speaks to a key feature of depression and anxiety – avoidance of new or stressful situations.
Poor mental health increases refusal rates for jobs outside the home, but not at home
Our first key finding is that poor mental health (both anxiety and depression) is strongly associated with a reduced willingness to take up this attractive work opportunity. As seen in the figure below, participants who are anxious and depressed (i.e. scoring above the PHQ and GAD thresholds) are roughly 54% more likely to decline the offered work than those who are neither anxious nor depressed (11.9% vs. 7.7%).
Figure 1: Mental health and work offer refusal rates
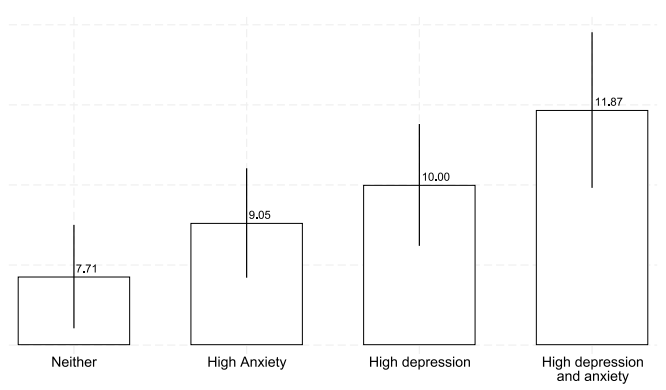
Notes: The bar heights show the percentage of participants who refuse the work offer, pooling across questions about work from home and work outside of the home (N=982). The spikes correspond to the standard errors of the means. High anxiety corresponds to a GAD-2 score of three or more. High depression corresponds to a PHQ-2 score of three or more.
These differences are not due to existing work obligations: more depressed individuals are less likely to cite existing work as a reason to decline and more likely to cite inability or unwillingness to take up the work as the reason for refusal. Nor do these differences in take-up appear to be driven by childcare responsibilities: respondents in poor and good mental health have similar numbers of young children.
However, this strong association between depression and anxiety and the willingness to work is only present for work offered outside of the home; correlations between either aspect of mental health and willingness to work from home are small in magnitude and statistically insignificant. This stark difference in take-up rates across work location for those in poor mental health is consistent with many of the symptoms of depression and anxiety – avoidance behaviours, low energy levels, nervousness or negative appraisals of novel situations – which could make individuals less willing to leave the home despite the relatively generous wages.
Phase 2: Productivity, income and quit rates for jobs at home
In the second phase of our study, conducted with the subsample of women willing to work from home, we randomly assign participants to two groups: those that are offered to work from home (treated) and those that are not offered any work (control). The randomisation allows us to examine whether, conditional on being willing to take up a job working from home, this random job offer is equally valuable to depressed and anxious individuals. In other words, among those willing to take up the work (which is not selected based on mental health status), do those with poor mental health have similar labour supply, output, earnings, and quit rates?
Unsurprisingly given that little work is available in the lean season, this random job offer greatly increases the likelihood of work among those offered the job, nearly quadrupling engagement with self-reported wage labour from 17% to 60% over the three months of work offered. We find that, although we cannot rule out small effects, in this group, depressed and/or anxious individuals are just as likely to supply labour, produce as much, and earn similar amounts as those in better mental health. Further, poor mental health does not predict quit rates overall.
In short, we conclude that depression and anxiety impede labour market success not only via lower productivity at work in traditional (outside of the home) work contexts (Ridley et al. 2020, Lund et al. 2019), but also because those with mental health conditions are much less likely to take up new labour opportunities. However, among individuals who take up home-based work – an outcome that is uncorrelated with baseline mental health – mental health does not reduce labour supply, output, or earnings, nor does it increase quit rates once they are on the job.
Policy implications for mental health, labour markets and cash-for-work programmes
Our results indicate that the association between poor mental health and reduced job take-up depends on the job environment: while depression and anxiety strongly predict lower acceptance of outside-the-home work opportunities, these same mental health conditions show no association with willingness to accept work-from-home positions. Further, among those who accept work-from-home positions, we find no evidence that mental health affects productivity, labour supply, or retention. This contrasts with existing evidence on mental health’s effects in traditional workplace settings and opens the door to an alternative way to successfully engage those in poor mental health in the labour market.
Next, while much of the work trying to explain low labour force participation in low- and middle-income countries has focused on demand-side constraints, such as job availability and search frictions, or supply-side factors, like skills and transportation costs, we highlight a mechanism through which poor mental health may create additional barriers to labour force entry. Our evidence demonstrates that even when attractive job opportunities are directly offered, poor mental health – which is highly prevalent in this context – substantially reduces take-up in traditional employment opportunities outside of the home, suggesting an important but previously overlooked constraint on engagement with the labour force.
Finally, we provide evidence on cash-for-work programmes, which are widely used as anti-poverty tools in low-income countries (Besley and Coate 1992, Bertrand et al. 2021, Murgai et al. 2016, Imbert and Papp 2015). These programmes typically operate through standing job offers outside of the home, assuming that those most in need will self-select into the work. Our findings suggest that poor mental health – which is disproportionately prevalent among the poor – may limit engagement with these programmes precisely among those they are intended to help. This has important implications for programme design: screening for mental health conditions and providing complementary mental health interventions or innovating to provide other targeted intervention designs such as work from home arrangements, may be necessary to achieve the full potential of cash-for-work as an anti-poverty tool.
References
Barker, N, G Bryan, D Karlan, A Ofori-Atta, and C Udry (2022), "Cognitive behavioral therapy among Ghana's rural poor is effective regardless of baseline mental distress," American Economic Review: Insights, 4(4): 527–545.
Bertrand, M, B Crépon, A Marguerie, and P Premand (2021), "Do workfare programs live up to their promises? Experimental evidence from Côte d'Ivoire," Unpublished manuscript.
Besley, T, and S Coate (1992), "Workfare versus welfare: Incentive arguments for work requirements in poverty-alleviation programs," American Economic Review, 82(1): 249–261.
Biasi, B, M S Dahl, and P Moser (2021), "Career effects of mental health," Unpublished manuscript.
Carvalho, L, D de Walque, C Lund, H Schofield, V Somville, and J Wei (2026), "Psychological barriers to participation in the labor market: Evidence from rural Ghana," Journal of Development Economics, 181: 103734.
de Quidt, J, and J Haushofer (2016), "Depression for economists," Unpublished manuscript.
Hakulinen, C, M Elovainio, M Arffman, S Lumme, S Pirkola, I Keskimäki, K Manderbacka, and P Böckerman (2019), "Mental disorders and long-term labour market outcomes: Nationwide cohort study of 2 055 720 individuals," Acta Psychiatrica Scandinavica, 140(4): 371–381.
Imbert, C, and J Papp (2015), "Labor market effects of social programs: Evidence from India's employment guarantee," American Economic Journal: Applied Economics, 7(2): 233–263.
Lund, C, S Docrat, J Abdulmalik, A Alem, A Fekadu, O Gureje, D Gurung, D Hailemariam, Y Hailemichael, C Hanlon, M J D Jordans, D Kizza, S Nanda, S Olayiwola, R Shidhaye, N Upadhaya, G Thornicroft, and D Chisholm (2019), "Household economic costs associated with mental, neurological and substance use disorders: A cross-sectional survey in six low- and middle-income countries," BJPsych Open, 5(3): e34.
Lund, C, K Orkin, M Witte, J H Walker, T Davies, J Haushofer, S Murray, J Bass, L Murray, W Tol, and V H Patel (2024), "The effects of mental health interventions on labor market outcomes in low- and middle-income countries," Unpublished manuscript.
Mojtabai, R, E A Stuart, I Hwang, R Susukida, W W Eaton, N Sampson, and R C Kessler (2015), "Long-term effects of mental disorders on employment in the National Comorbidity Survey ten-year follow-up," Social Psychiatry and Psychiatric Epidemiology, 50(11): 1657–1668.
Murgai, R, M Ravallion, and D van de Walle (2016), "Is workfare cost-effective against poverty in a poor labor-surplus economy?," World Bank Economic Review, 30(3): 413–445.
Ridley, M, G Rao, F Schilbach, and V Patel (2020), "Poverty, depression, and anxiety: Causal evidence and mechanisms," Science, 370(6522): eaay0214.
World Health Organization (2022), "World mental health report: Transforming mental health for all."