




The end of guerrilla violence in Colombia reshaped the composition of healthcare workers in conflict-affected areas. Despite redistributing healthcare workers away from these areas, they maintained service quality, offering valuable insights for public services in post-conflict settings.
The World Health Organization (WHO) projected a global deficit of 11 million healthcare workers (HCWs) by 2030, mainly affecting low- and lower-middle-income countries (WHO 2025). This may be a lower bound, as other studies estimate almost 15 million (Liu et al. 2017). Regardless of the figure, the projected scarcity of HCWs is an extraordinary global challenge. But it is also a problem that affects specific countries, as unequal access to HCWs across regions with different levels of urbanisation and development remains a pressing issue.
While much of the global health workforce agenda focuses on the role of training and task reallocation, less is known about how large-scale political transitions—such as the end of armed conflict—reshape the geography and composition of HCWs. Understanding how peace affects public sector labour markets is increasingly relevant for countries recovering from violence. Our research contributes to this emerging agenda by demonstrating how the end of conflict changes not only the quantity but also the spatial distribution and productivity of health workers. In addition to the public health evidence on resource composition (WHO et al. 2007), our research contributes to existing work on the personnel economics of the state, especially in developing countries (Dal Bó et al. 2013, Ashraf et al. 2014, Finan et al. 2017), as well as the fragility of service provision under weak state control (Berman et al. 2011, Okunogbe and Tourek 2024).
Could ending a conflict encourage healthcare workers to move to previously violent areas? While many would expect improved living conditions to attract additional healthcare workers, our research tells a different story. Following the unilateral ceasefire declared by the Revolutionary Armed Forces of Colombia (FARC) in December 2014, during peace negotiations with the government, conflict-affected rural areas lost healthcare workers—despite this, the quality of care did not worsen.
This unexpected pattern suggests that peace reshapes healthcare delivery not only through new funding or reforms, but by reassigning who goes where. As mobility restrictions are lifted, health workers freely reallocate across space. In Colombia, this led to a leaner but more productive rural workforce, with no deterioration of health outcomes.
This sheds light on the often-overlooked observation that, as illegal territorial governance entails mobility restrictions in the form of curfews or checkpoints, conflict termination can lead to a reallocation of service providers, which may help or slow down post-conflict recovery, depending on contextual factors.
Studying the impact of conflict on public service provision
Colombia’s internal conflict lasted more than fifty years. In many rural areas with high levels of FARC violence, mobility was heavily restricted. Checkpoints, threats, and insecurity kept healthcare workers from leaving. The permanent ceasefire declared by FARC in December 2014, amid peace negotiations with the government, changed that. Violence plummeted, road access improved, and relocation became feasible.
Using annual administrative data from Colombia’s health system (2011-2018), we examined how this shift affected the geographic distribution and composition of the health workforce (Mora-García et al. 2025). Our key finding: municipalities with high FARC violence before the ceasefire saw a 13.4% greater reduction in healthcare workers per 1,000 people relative to other areas. This reduction was not driven by population loss or changes in healthcare budgets; instead, it reflected the reallocation of health workers once mobility constraints disappeared.
We identify these effects using a difference-in-differences strategy, comparing across municipalities with varying levels of pre-ceasefire FARC violence, before and after the December 2014 ceasefire. We use annual employment records from Colombia’s social security system and the Ministry of Health’s registry of healthcare workers. This allows us to track employment levels, qualifications, and locations over time. Crucially, we control for population, insurer behaviour, and patient demand to isolate the effects of the ceasefire.
Controlling for municipality trends, regional shocks, and changes in infrastructure or population, we rule out alternative explanations such as changes in patient demand or insurer behaviour. Our evidence consistently points to increased mobility, enabled by peace, as the key driver.
Conflict-affected rural areas lost workers, but maintained care quality
The reduction was concentrated among vocational nurses and lower-skilled staff, who had been less mobile during the conflict (see Figure 1). Physicians and more highly trained workers were more likely to remain. Municipalities exposed to a one standard deviation increase in FARC violence experienced a 14–16% decline in the share of vocational nurses and nurses overall post-ceasefire. The reduction in physicians was smaller, at around 7%. This compositional shift meant that while the overall number of healthcare workers declined, the remaining workforce was, on average, more qualified.
Despite fewer workers, the quality of care did not decrease. Mortality rates remained stable. Physician-led services, such as cervical cancer screening increased slightly (municipalities with a one standard deviation increase in FARC violence saw a 5.4% increase in standard breast cancer screenings (bilateral mammograms) for women aged 50 to 69, per 1,000 residents). Although services more reliant on nurses, such as diabetes and cholesterol testing, declined modestly (2-3%), overall healthcare provision adapted to these new staffing realities. These patterns suggest that productivity increased, as a smaller workforce maintained—and in some cases improved—levels of service delivery.
Figure 1: Effect of the FARC ceasefire on health workforce density
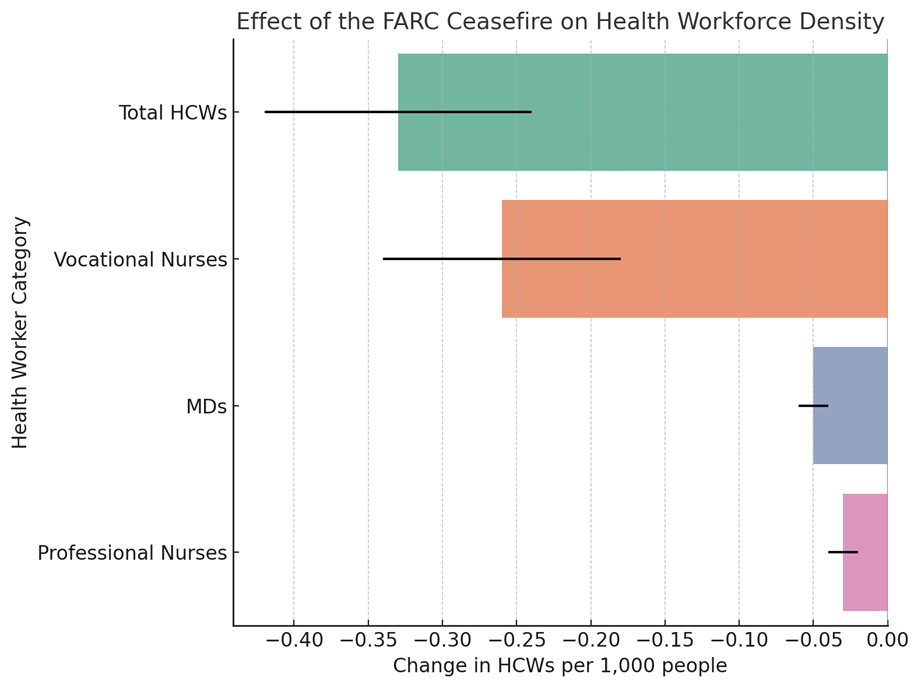
Note: Own calculations with the coefficients of Table 2 in Mora-García et al (2025).
Policy implications for post-conflict mobility and service delivery
Our findings offer three key lessons for policymakers in fragile or post-conflict settings:
- Do not assume automatic improvements after conflict ends: Some areas may lose personnel once security improves and mobility is restored.
- Reallocation matters: Improvements in service delivery may come not just from hiring or investment, but from changes in workforce distribution.
- Anticipate and manage transitions: Peace can trigger rapid shifts in personnel, particularly in rural or formerly isolated areas. Planning for this reallocation is essential to preserve service quality.
Ending conflict does more than stop violence—it alters the constraints that shape how public systems operate. In Colombia, peace triggered a spatial reallocation of healthcare workers. Conflict-affected rural areas lost staff but maintained service quality through shifts in composition and productivity. This highlights how systems adapt to changes in constraints and opportunities. Understanding these dynamics is key for countries transitioning out of conflict and aiming to build resilient public services.
References
Ashraf, N, O Bandiera, and B K Jack (2014), “No margin, no mission? A field experiment on incentives for public service delivery,” Journal of Public Economics, 120: 1–17.
Berman, E, J N Shapiro, and J H Felter (2011), “Can hearts and minds be bought? The economics of counterinsurgency in Iraq,” Journal of Political Economy, 119(4): 766–819.
Dal Bó, E, F Finan, and M A Rossi (2013), “Strengthening state capabilities: The role of financial incentives in the call to public service,” The Quarterly Journal of Economics, 128(3): 1169–1218.
Finan, F, B A Olken, and R Pande (2017), “The personnel economics of the developing state,” in Handbook of Economic Field Experiments, 2: 467–514.
Liu, J X, Y Goryakin, A Maeda, T Bruckner, and R Scheffler (2017), “Global health workforce labor market projections for 2030,” Human Resources for Health, 15: 1–12.
Mora-García, C, M Prem, P Rodríguez-Lesmes, and J F Vargas (2025), “Health workforce reallocation in the aftermath of conflict: Evidence from Colombia,” Labour Economics, 102710.
Okunogbe, O, and G Tourek (2024), “How can lower-income countries collect more taxes? The role of technology, tax agents, and politics,” Journal of Economic Perspectives, 38(1): 81–106.
World Health Organization (WHO) (2025), "Health workforce".
World Health Organization (WHO), PEPFAR, and UNAIDS (2007), "Task shifting: Rational redistribution of tasks among health workforce teams – Global recommendations and guidelines".