






A careful examination of Nestlé’s marketing behaviour shows that Nestlé’s entry into low- and middle-income formula markets caused about 212,000 infant deaths per year among mothers without clean water access at the peak of the Nestlé controversy in 1981
While substitutes for breastmilk have existed since time immemorial, infant formula as it is known today is a relatively recent invention. It was first developed in Germany in 1865 and marketed as a medically endorsed product “closest to mother’s milk” (Stevens et al. 2009), becoming popular during the Industrial Revolution given the large number of women who were leaving home to enter the labour market. Infant formula use rose steadily in subsequent decades, peaking during the post-World War II baby boom (Akhter 1994), after which sales began to decline in higher income countries due to lower birth rates and a growing belief in the positive health effects of breastfeeding (Stevens et al. 2009).
Formula producers searching to offset declining sales thus turned to other markets, expanding into the developing world in the 1960s and 70s. For example, Nestlé annual reports from the early 1960s note the firm’s growing market for infant formula in South Africa under the Lactogen brand name:
“Increased sales of Lactogen reflect the growing awareness amongst African races of the need for improving the nutrition of young children.” (Nestlé (2018), 1961, p.10)
“The native population is realizing more than ever the practical advantages and nutritional value of the milk specialties in the infant food range, which established new records over the past year.” (Nestlé (2018), 1962, p.14)
The introduction of infant formula into low- and middle-income country (LMIC) markets has since become one of the most notorious corporate controversies. Nestlé emerged at the center of the controversy because the company was accused of unethical marketing practices (Dobbing and Falkner 1988), and because it was both an early entrant into LMIC markets and by far the largest infant formula supplier worldwide. Infant formula companies, in particular Nestlé, began aggressively marketing infant formula as scientific, modern, prestigious, and (falsely) nutritionally superior to breastmilk (Hicks 1981). Nestlé was accused of providing free or low-cost supplies of infant formula in hospitals and maternity centers, often dispensed by “milk nurses” (saleswomen dressed in nurses uniforms) to encourage new mothers to use infant formula (Jelliffe 1975, Gilly and Graham 1988, Austin 2008). Formula use among newborns increases the risk that mothers release prolactin-inhibiting hormones, which signal milk production to shut down, creating a future dependence on breastmilk substitutes (Latham 1977). By the 1960s, Nestlé already viewed marketing of formula in hospitals as a strategic approach to encouraging adoption of infant formula, as seen in an excerpt from its 1969 annual report:
“... some factors are more favorable such as the increased buying power in the developing countries, and the rising number of births in maternity hospitals where it is easier to reach mothers. This is due to the fact that the medical staff there is more likely to influence mothers with regard to the food most suitable for their babies.” (Nestlé (2018), 1969, p.16)
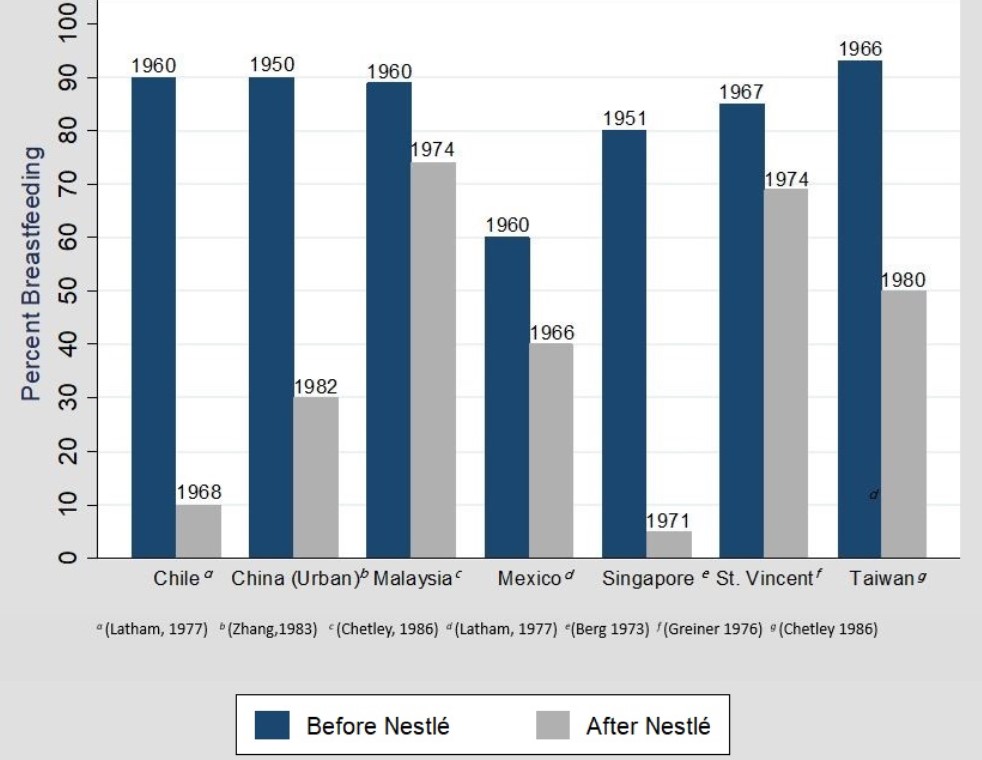
By the mid-1970s, public health activists began to warn of large numbers of “formula-induced” infant deaths in LMICs (Jelliffe 1975). Many in the public health community accused the infant formula firms of promoting formula to mothers in LMICs who were unlikely to have access to clean water sources and sufficient knowledge of nutrition, physiology, or mechanisms of disease transmission to prevent the health risks associated with formula contamination (Dobbing and Falkner 1988). Likewise, concern arose over the decline in breastfeeding associated with the introduction of infant formula across LMICs (Kent 2015). Indeed there is evidence that the introduction of infant formula into a country’s market was correlated with a substantial reduction in breastfeeding. Latham (1977), for example, documents the dramatic decline in breastfeeding in Chile, where breastfeeding declined from 90% of all children in 1960 to only 10% by 1968 after the introduction of formula.
Figure 1: Decline in breastfeeding with formula introduction
There are two primary channels through which formula could plausibly affect infant mortality. First, the increased use of infant formula could cause a decline in breastfeeding (Pérez-Escamilla et al. 2023). There is a strong consensus that the substitution of formula for breastmilk compromises a child’s physical health and immune response (Victora et al. 2015). Based on the evidence linking breastfeeding to better child development outcomes, the World Health Organization (WHO) recommends that infants be breastfed within the first hour of birth, exclusively breastfed for the first 4-6 months of life, and continue to receive breastmilk (alongside complementary foods) for up to two years of age (WHO 2009). However, less than half of newborns worldwide are breastfed within an hour of birth, and only 44% are exclusively breastfed from birth to 6 months (Keeley 2021). While there are many other reasons a mother may rationally choose to use infant formula instead of breast-feeding, including working outside the home, the inability to pump or store breast milk, lack of family support, and a host of other socio-cultural and structural factors (Balogun et al. 2016, Bazzano et al. 2017, Beasley and Amir 2007), misinformation on the “nutritional value” of formula consumption for children relative to breastfeeding (and lack of information provision on the health benefits of breastfeeding) may have created a particularly large distortion in mothers’ decision-making.
Second, the public health literature has noted the risk from caregivers mixing infant formula powder with unclean water (Dobbing and Falkner 1988), resulting in bacterial infection and diarrheal disease that increases the risk of infant mortality through sickness and dehydration (Pérez-Escamilla et al., 2023). Given the high prevalence of exposure to unclean water sources in LMICs, there are clear pathways connecting poor quality water with poor infant health outcomes (Marino 2007, VanDerslice et al. 1994, Weisstaub and Uauy 2012, Schuster et al. 2020). These problems may be elevated among caregivers with low literacy who may have difficulty understanding directions on packaging labels, putting infant lives at risk (Muller 1975).
In our research (Anttila-Hughes et al. 2023), we provide the first population-level evidence exploring these claims by estimating the casual effect of Nestlé’s marketing of infant formula on infant mortality in LMICs. We do so by assembling a dataset with over 2.6 million infant births and deaths across 38 countries from the Demographic and Health Surveys (DHS), matching children’s year of birth to data on the timing of Nestlé entrance into country infant formula markets collected from the Nestlé corporation’s annual investor reports (Nestlé 2018). Since Nestlé was the largest and typically the first international formula producer to enter LMIC markets during the 20th century (Dobbing and Falkner 1988), its entry into a country’s market represents a substantial increase in the availability of infant formula. Nestlé’s extremely detailed records of their operations in their annual reports further provide precise information on when individual countries were exposed to the market segment containing formula itself, allowing us to reconstruct their global activities from 1966 onwards.
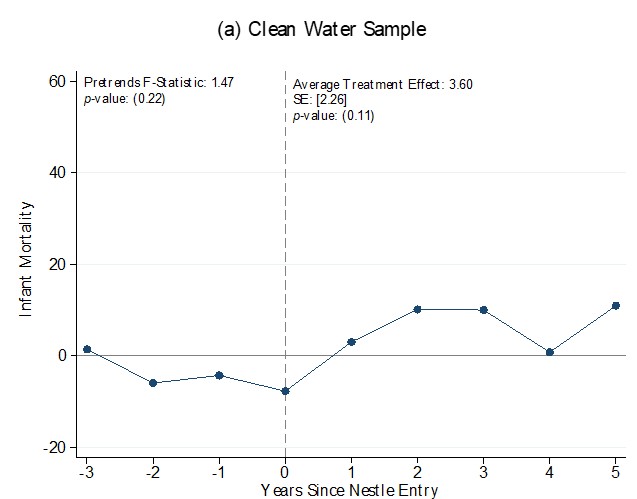
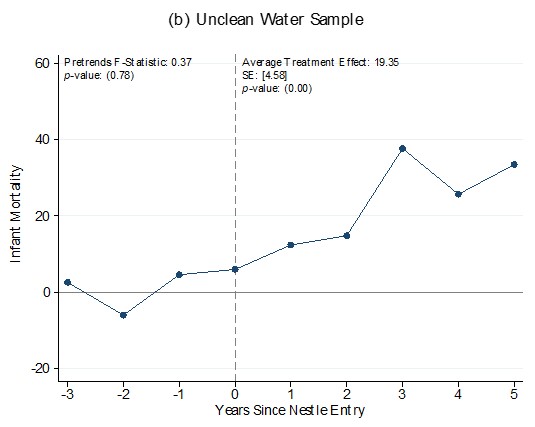
In order to distinguish between plausible mortality channels, we conduct separate analyses for households that had access to clean versus unclean sources of water. An increase in mortality among households in both samples would be consistent with reduced breastfeeding, driving effects on infant mortality. On the other hand, if contaminated water is the primary risk, then mortality effects should be concentrated in households using unclean water, consistent with concerns that formula prepared with unclean water acts as a vector for enteric diseases.
We find sharp increases in infant mortality after Nestlé’s entrance into LMIC formula markets, but only in households with unclean water. We estimate that mortality risk for a child born in the 5 years after Nestlé market entry increases by 19.35 per 1000 live births, an increase of 27% over the baseline mortality rate in the unclean water sample. We do not find a similar increase in the clean water sample, indicating that whatever the health costs of switching from breastfeeding to formula, poor sanitation is the principal driver of mortality risk.
Figure 2: Child mortality after Nestlé market entry
Together these results paint a picture of strikingly large increases in infant mortality caused by the introduction of formula into markets where access to clean water is not universal. We estimate that Nestlé’s entry into LMIC formula markets caused about 212,000 infant deaths per year among mothers without clean water access at the peak of the Nestlé controversy in 1981, and has led to approximately 10.9 million excess infant deaths between 1960 and 2015.
One message that emerges from our analysis is the critical importance of making sure that parents who use formula, use it safely. Clear instructions comprehensible to mothers of all education levels need to be included in marketing and packaging materials. In regions where many households do not have access to clean water, infant formula companies may consider pre-mixing formula with clean water, or perhaps including chlorine tablets with formula packaging.
At the same time, formula firms themselves clearly must be held responsible for their marketing decisions. Compliance with the International Code of Marketing Breastmilk Substitutes (ICMBS) (WHO, 1981) remains voluntary, and banned marketing practices continue. In fact, a recent systematic review reported inappropriate marketing by formula companies in 95 countries and all WHO regions across a range of settings, including health systems, public spaces, points of sale, media, emergency programmes and direct to mothers (Becker et al. 2022). The documented violations include promotional claims that mislead consumers and surreptitious methods to influence doctors and other health professionals, such as sponsoring medical conferences and partnering with health-promoting NGOs, misleading and inaccurate health claims, along with the growing use of social media and other digital platforms. To combat these abuses, WHO, UNICEF and the International Baby Food Action Network have called for countries to enact ICMBS legislation with stringent enforcement mechanisms and penalties for nonadherence, to closely monitor adherence (WHO 2018), and to increase focus on new digital marketing strategies and differentiated types of breastmilk substitutes and associated products (Becker et al. 2022). Exactly how such efforts will play out, and what their ultimate impact on infant heath will be, remain to be seen.
References
Akhter, S H (1994), “Multinational corporations and the impact of public advocacy on corporate strategy: Nestlé and the infant formula controversy.”
Anttila-Hughes, J K, L C Fernald, P J Gertler, P Krause, E Tsai, and B Wydick (2023), “Mortality from Nestlé’s marketing of infant formula in low and middle-income countries” NBER Working Paper 24452.
Austin, J E (2008), Strategic management in developing countries. Simon and Schuster.
Baker, M and K Milligan (2008), “Maternal employment, breastfeeding, and health: Evidence from maternity leave mandates.” Journal of Health Economics 27(4): 871–887.
Balogun, O O, S Kobayashi, K M Anigo, E Ota, K Asakura, and S Sasaki (2016), “Factors influencing exclusive breastfeeding in early infancy: a prospective study in north central Nigeria.” Maternal and Child Health Journal 20(2): 363–375.
Bazzano, A N, A Kaji, E Felker-Kantor, L A Bazzano, and K S Potts (2017), “Qualitative studies of infant and young child feeding in lower-income countries: a systematic review and synthesis of dietary patterns.” Nutrients 9(10): 1140.
Beasley, A and L H Amir (2007), Infant feeding, poverty and human development.
Becker, G E, P Zambrano, C Ching, J Cashin, A Burns, E Policarpo, J Datu-Sanguyo, and R Mathisen (2022), “Global evidence of persistent violations of the international code of marketing of breast-milk substitutes: A systematic scoping review.” Maternal & Child Nutrition 18, e13335.
Dobbing, J and F Falkner (1988), Infant feeding: anatomy of a controversy, 1973-1984. Springer.
Gilly, M C and J L Graham (1988), “A macroeconomic study of the effects of promotion on the consumption of infant formula in developing countries.” Journal of Macromarketing 8(1): 21–31.
Hicks, G M (1981), “The infant formula controversy.” Backgrounder 142: 1–9.
Jelliffe, D B (1975), Advertising and infant feeding.
Keeley, B (2021), “The State of the World’s Children 2021: On My Mind–Promoting, Protecting and Caring for Children’s Mental Health.” ERIC.
Kent, G (2015), “Global infant formula: monitoring and regulating the impacts to protect human health.” International Breastfeeding Journal 10(1): 1–12.
Latham, M C (1977), “Infant feeding in national and international perspective: an examination of the decline in human lactation, and the modern crisis in infant and young child feeding practices.” Annals of the New York Academy of Sciences 300(1): 197–209.
Marino, D D (2007), “Water and food safety in the developing world: global implications for health and nutrition of infants and young children.” Journal of the American Dietetic Association 107(11): 1930–1934.
Muller, M (1975), “The baby killer; A War on Want investigation into the promotion and sale of powdered baby milks in the Third World.” Available here.
Nestlé (1960–2018). Annual reports. Available here: https://www.nestle.com/investors/publications.
Pérez-Escamilla, R, C Tomori, S Hernández-Cordero, P Baker, A J Barros, F Bégin, D J Chapman, L M Grummer-Strawn, D McCoy, P Menon, et al. (2023), “Breast- feeding: crucially important, but increasingly challenged in a market-driven world.” The Lancet 401(10375): 472–485.
Stevens, E E, T E Patrick, and R Pickler (2009), “A history of infant feeding.” The Journal of Perinatal Education 18(2): 32–39.
VanDerslice, J, B Popkin, and J Briscoe (1994), “Drinking-water quality, sanitation, and breast-feeding: their interactive effects on infant health.” Bulletin of the World Health Organization 72(4): 589.
Victora, C G, B L Horta, C L De Mola, L Quevedo, R T Pinheiro, D P Gigante, H Gonçalves, and F C. Barros (2015), “Association between breastfeeding and intelligence, educational attainment, and income at 30 years of age: a prospective birth cohort study from Brazil.” The Lancet Global Health 3(4): e199–e205.
Weisstaub, G and R Uauy (2012), “Non-breast milk feeding in developing countries: challenge from microbial and chemical contaminants.” Annals of Nutrition and Metabolism 60(3): 215–219.
WHO (1981), “International code of marketing of breast-milk substitutes.” World Health Organization and others.
WHO (2009), “Infant and young child feeding: model chapter for textbooks for medical students and allied health professionals.” World Health Organization and others.
WHO (2018), “Marketing of breast-milk substitutes: National implementation of the inter- national code, status report 2018.”