


A three-day training programme to improve hairdressers’ active listening skills did not improve women’s mental health in Abidjan, Côte d’Ivoire, and in fact worsened mental health outcomes for providers. However, the training did change women’s perception of mental health, associating it more with disease and less with being ‘crazy’.
Women have limited access to mental health services in Côte d’Ivoire
Mental health disorders represent a growing global health crisis, disproportionately affecting women (Dattani et al. 2023). The WHO estimates that mental health problems are among the leading contributors to years lived with disability in Africa (WHO 2022). Despite the substantial economic and social effects, care for mental illnesses remains severely underfunded in the developing world (Gilbert et al. 2015, Ridley et al. 2020), with little progress towards building robust mental health infrastructure. For instance, Côte d’Ivoire counts fewer than one mental health professional per 100,000 inhabitants (Ridley et al. 2020). This supply-side constraint is compounded by what has been termed a ‘care gap’ (Pathare et al. 2018, Patel et al. 2018), reflecting deeply rooted stigma and persistent scepticism around mental illness and its treatment. While 33.3% of individuals report having experienced an episode of depression or anxiety affecting their regular daily activities for more than two weeks in Côte d’Ivoire in 2020, only 22.7% of the total population express confidence in scientific treatment (Wellcome Global Monitor 2021).
Efforts to address the mental health treatment gap must therefore go beyond increasing clinical capacity, building on the potential of task-sharing models—in which trained non-specialists deliver basic mental health support. Research has demonstrated the effectiveness of simplified psychotherapeutic interventions such as cognitive behavioural therapy and interpersonal therapy in reducing symptoms of depression and anxiety when delivered by non-specialist providers (Singla et al. 2017, Baranov et al. 2020, Baird et al. 2025). However, critical gaps remain in understanding how to deliver these services in safe and accessible spaces, especially for women in fragile and low-trust environments.
Training local service providers to be first responders for mental health
Our research assessed the impact of an innovative pilot training local service providers (in this case, hairdressers) to become a first line of defence against mental illness in low-income settings (Nilsson and Pougué Biyong 2025). The Heal-by-Hair programme, implemented by the Bluemind Foundation, aims to improve the socio-emotional skills and well-being of hairdressers and customers, producing positive externalities in women’s economic empowerment outcomes.
During the three-day training, individuals received information and participated in role-playing exercises mimicking everyday conversations that may arise in interactions with their customers. Hairdressers were trained by medical professionals coming from or working in West African countries, of which seven out of nine were women. The training aimed to provide a skillset encompassing cognitive, affective, and behavioural processes critical to active listening as mental health support (Stickley and Freshwater 2006, Jones et al. 2019). Hairdressers were not expected to provide medical care but instead received guidance on how to be more empathetic to customers, recognise mental health issues, and, if necessary, refer their customers to appropriate caregivers. Hairdressers also attended monthly therapeutic sessions and were added to a WhatsApp group after completing the training. Although the training was a one-time intervention, hairdressers continued to engage with the NGO over time. These ongoing interactions were intended to help keep their acquired knowledge fresh and stimulate increased confidence among hairdressers through sharing of cases.
We evaluated the impact of this programme using a randomised control trial with two follow-ups at 6 and 18 months. The sample initially targeted 300 hairdressers and 1,500 customers, with half of the hairdressers randomly assigned to a control group and the other half assigned to the active-listeners training group. However, due to low baseline response rates, we opted to interview additional clients after baseline. The study enrolled 247 hairdressers at baseline, of whom 150 were invited to training and 74 attended, yielding a 49.3% take-up rate. Of the 786 baseline customers, 475 participated in the first follow-up and 493 new ones were added, totalling 968 at the first follow-up. One year later, 852 customers were re-interviewed, reflecting an 88% retention rate between the two follow-ups.
Training improved hairdresser-customer relationships in the medium term
Our results show that hairdresser-customer interactions improved in the medium term, but not in the short term. After 18 months, trained hairdressers reported an increase in the frequency with which customers shared their private lives, as well as customers’ willingness to talk about difficulties and hairdressers’ ability to provide relevant support in these cases. Figure 1 presents these estimates, suggesting that hairdressers did feel somewhat empowered in their ability to provide moral support to customers. Consistent with the goals of the Heal-by-Hair programme, this indicates that hairdressers altered their approach to interacting with customers, increasing their willingness to share, and hairdressers felt more confident in their ability to help. The training gives hairdressers the skills to provide a safe space for customers. This enhanced support role is evident in customers citing hairdressers’ ‘human qualities’ as a reason for their visit 18 months later. While this suggests that customers may have perceived a shift in their relationship with the hairdresser post-training, other outcomes were not statistically significant.
Figure 1: The effects of the Heal-by-Hair programme on hairdresser-customer interactions at 18 months
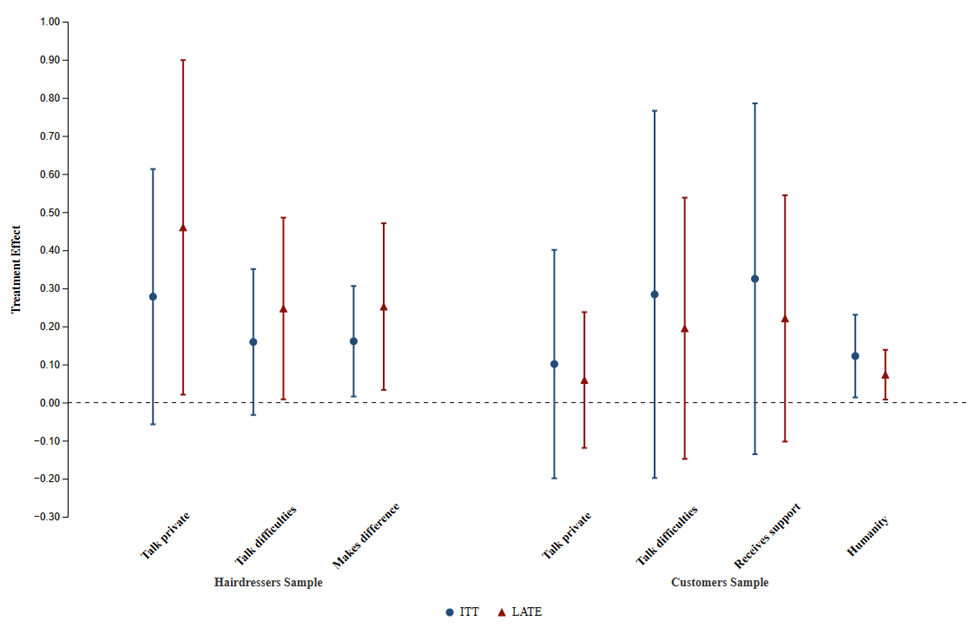
Note: The figure depicts the Intention-to-Treat and the Local Average Treatment Effect. The trained hairdressers reported a 0.5 standard deviation (LATE) increase in the frequency with which customers shared their private lives, and 0.25 standard deviation (LATE) increase in customers’ willingness to talk about difficulties and hairdressers’ ability to provide relevant support in these cases. The customers of trained hairdressers reported a 0.07 increase in hairdressers’ humanity (LATE). Dots are point estimates and horizontal lines are 90% confidence intervals.
Training did not improve customers’ well-being, but did change their representations of mental health disorders
We measure hairdresser and customer well-being and mental health using the WHO-5 Well-Being Index, PHQ-9 index for depression, and self-declaration of mental problems. We find that trained hairdressers were more likely to report experiencing a mental health problem after six months than their untrained counterparts, both in terms of PHQ-9 scores and self-declared mental illnesses. Moreover, despite more supportive conversations, customers’ psychometric scales did not show any significant improvement post-intervention. However, customers with self-reported mental health problems that have a trained hairdresser are more likely to have discussed it with someone than those without one.
The surprising and apparent worsening of mental health may be linked to reduced stigma and a shift in awareness regarding what constitutes a mental health problem. We tested the hypothesis that limited knowledge of mental health may prevent individuals from conceptualising mental health disorders as a medical condition (Patel 1995). Our analysis of associated words further supports that hairdressers were more likely to associate mental health with ‘disease’ and that customers of treated hairdressers updated their understanding of mental health. Specifically, they were 44% more likely to associate mental health with mood disorders (‘depression’), and 34% less with psychotic illness (‘craziness’).
Lessons for mental health policy in developing countries
The Heal-by-Hair programme had weak but positive effects on hairdresser-customer interactions in the long-term, and stronger but negative effects on hairdressers’ PHQ-9 and self-assessed mental health issues in the short term, underscoring that awareness alone is insufficient without pathways to care. However, our results support empowering non-specialist mental health providers to reframe issues previously perceived as non-medical using a clinical framework, reshaping perceptions of mental health disorders.
We urge further research to explore in greater depth the connections between stigma, self-evaluative capacity, and actual mental illness in low-income settings. In addition, further approaches to scale-up community-based intervention should move beyond stand-alone training and be integrated into broader, resources-care ecosystems with safeguards for those offering support in order to yield sustained benefits.
References
Baird, S, B Özler, C Dell’Aira, L Parisotto, and D Us-Salam (2025), “Therapy, mental health, and human capital accumulation among adolescent girls in Uganda,” Journal of Development Economics 176: 103473.
Baranov, V, S Bhalotra, P Biroli, and J Maselko (2020), “Maternal depression, women’s empowerment, and parental investment: Evidence from a randomized controlled trial,” American Economic Review 110(3): 824–859.
Dattani, S, L Rodés-Guirao, H Ritchie, and M Roser (2023), “Mental health,” Our World in Data.
Gilbert, B, V Patel, P Farmer, and C Lu (2015), “Assessing development assistance for mental health in developing countries: 2007–2013,” PLoS Medicine 12(6): e1001834.
Jones, S, G Bodie, and S Hughes (2019), “The impact of mindfulness on empathy, active listening, and perceived provisions of emotional support,” Communication Research 46(6): 838–865.
Nilsson, B, and C Pougué Biyong (2025), “Hairdressers and well-being: Local services provision and mental health first response,” Journal of Development Economics: 103528.
Patel, V (1995), “Explanatory models of mental illness in sub-Saharan Africa,” Social Science & Medicine 40(9): 1291–1298.
Patel, V, S Saxena, C Lund, G Thornicroft, F Baingana, P Bolton, et al. (2018), “The Lancet Commission on global mental health and sustainable development,” The Lancet 392(10157): 1553–1598.
Pathare, S, A Brazinova, and I Levav (2018), “Care gap: A comprehensive measure to quantify unmet needs in mental health,” Epidemiology and Psychiatric Sciences 27(5): 463–467.
Ridley, M, G Rao, F Schilbach, and V Patel (2020), “Poverty, depression, and anxiety: Causal evidence and mechanisms,” Science 370(6522): eaay0214.
Singla, D, B Kohrt, L Murray, A Anand, B Chorpita, and V Patel (2017), “Psychological treatments for the world: Lessons from low- and middle-income countries,” Annual Review of Clinical Psychology 13(1): 149–181.
Stickley, T, and D Freshwater (2006), “The art of listening in the therapeutic relationship,” Mental Health Practice 9(5).
Wellcome Global Monitor (2021), “The role of science in mental health,” The Wellcome Trust.
World Health Organization (WHO) (2022), “World mental health report: Transforming mental health for all,” World Health Organization.