




Across Africa, early first-births remain the norm even as educational attainment has increased. Evidence from Zambia shows misperceptions and medical mistrust may be a key reason why.
When hormonal contraceptives became widely available in the US and Latin America, they transformed women’s lives. The pill allowed young women to delay first births, complete higher education, and pursue careers in far greater numbers. Economists have linked this shift to large gains in women’s earnings and labour force participation (Goldin and Katz 2002, Bailey 2006).
In sub-Saharan Africa, however, the revolution has not arrived. School enrolment has surged and access to modern contraceptives has expanded, yet early first-births remain widespread: six in ten women give birth before age 20 (Ahinkorah et al. 2021). Even among university students, where the returns to delaying may be particularly high, contraceptive use is strikingly low. Indeed, in the non-profit community, increasing contraceptive use among young childless women in sub-Saharan Africa is often considered difficult and prohibitively costly.
In a new randomised controlled trial at the University of Zambia, we explore one potential barrier to a sub-Saharan African contraceptive revolution (Bau, Henning, Low, and Steinberg 2025). We worked with 1,500 female students to test whether a pervasive and highly prevalent incorrect belief – that contraceptives cause infertility – prevents young women from using modern methods. Our results show that this belief is not only widespread but also impacts decision-making. When beliefs changed, contraceptive use rose and pregnancies fell.
A puzzling gap: Contraceptive use in Zambia
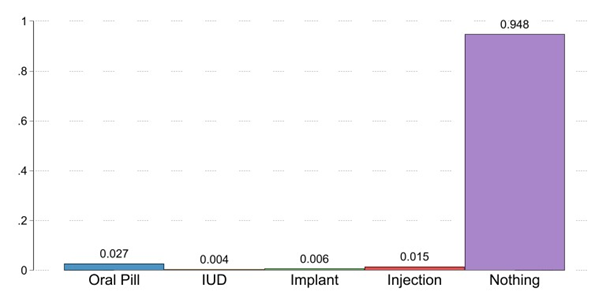
Our baseline survey painted a stark picture: 60% of female undergraduates reported having had sex, yet only 5% were using a hormonal contraceptive such as the pill, injection, or implant (see Figure 1). Moreover, this was not because young women were using condoms. Over six months of data collection, 41% of sexual encounters were condomless, and 58% of the sample had condomless sex at least once. Pregnancies were common, even though almost none of the students reported wanting to conceive while enrolled in school. Over the six months, 5.3% of the sample reported they were pregnant or tested positive for pregnancy at some point.
But this baseline data, along with qualitative focus groups, suggested that fear of infertility could be an important barrier to usage. Nearly two-thirds of women believed that at least one contraceptive method would make them unable to bear children later in life. This finding echoed a wide qualitative evidence base across Africa, where infertility concerns are consistently cited as a barrier to modern contraception (Boivin et al. 2020, Engelbert Bain et al. 2021).
This data motivates two central questions: (1) Could beliefs be shifted? (2) If so, would changing them increase contraceptive use?
Figure 1: Baseline contraceptive use among participants
Understanding the role of infertility fears
To answer these questions, we designed a randomised controlled trial with three arms. All participants attended a workshop on women’s health and received information about a partner clinic where contraceptives were available free of charge and without waiting.
One group only received this basic information. A second group was offered a travel voucher worth about US$4 that could be redeemed on visiting the clinic (whether or not the participant took up a method). This voucher reduced the cost of visiting the clinic and accessing contraceptives. A third group received the voucher plus an additional information session designed specifically to counter infertility fears.
The infertility session combined medical explanations with narratives by facilitators with a similar background to the participants. Facilitators explained how contraceptives temporarily pause ovulation, then shared their own stories of using contraception and later conceiving children. They showed photographs of their families and scars from contraceptive implants, providing vivid proof that fertility returns. The treatment was specifically designed to affect highly persistent, hard-to-change beliefs. Its design is in line with work showing that narratives can be more effective than bland statistics (Graeber et al. 2024) and that whether participants identify with the source of the information matters (Malmendier and Veldkamp 2022).
Receiving infertility information led to sustained contraceptive use
Students in the groups that received the voucher were more likely than the control group to visit the clinic. But only those who received infertility information adopted and continued using contraceptives over time.
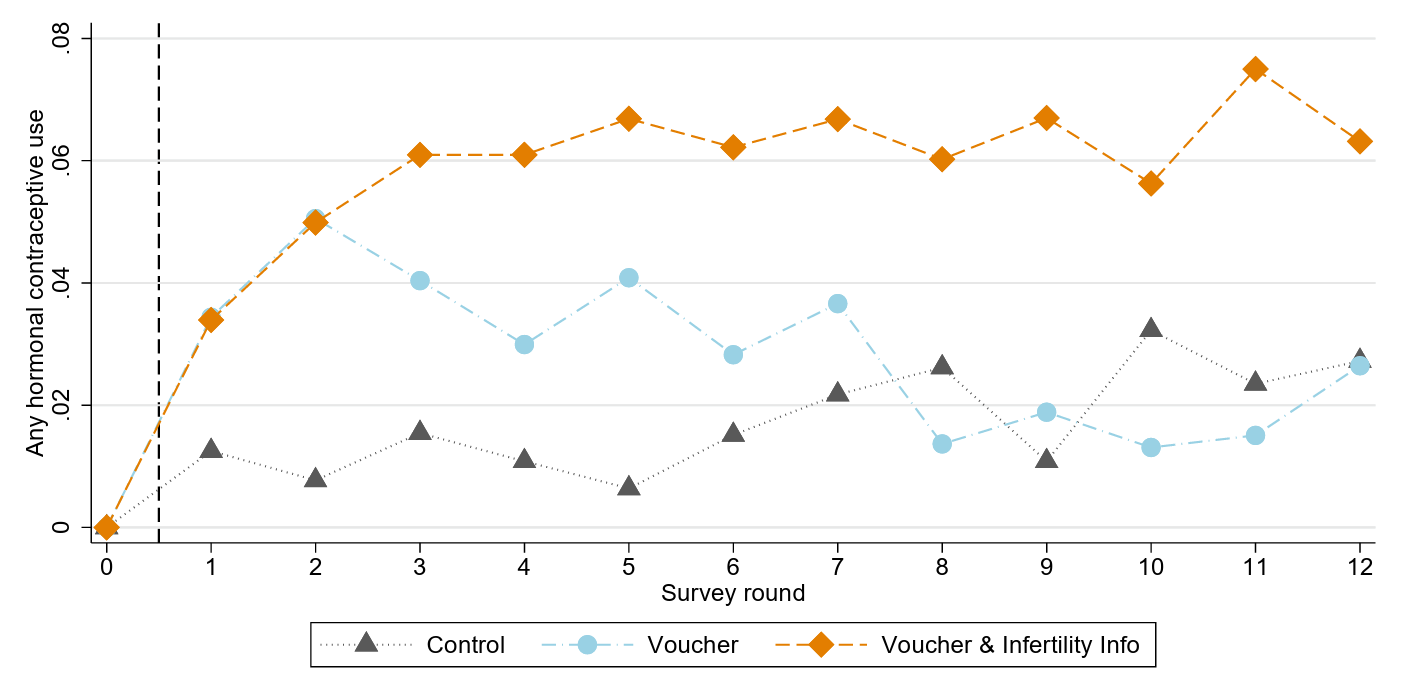
Immediately after the intervention, contraceptive take-up was higher in both voucher groups. Over time, however, the pattern diverged (see Figure 2). In the voucher-only group, contraceptive use fell back towards control levels within a month. By contrast, in the group that also received infertility information, use remained elevated and even grew over time. Six months later, women in this group were 40% more likely than the control group to be using a hormonal method. In part, this was due to switching to longer-lasting methods that are easier to use (the shot and implant) but may lead to greater concerns about infertility side effects (e.g. they are more invasive and affect the likelihood of having a period).
Pregnancy outcomes told a similar story. Pregnancies were much less common in the group that received infertility information, consistent with sustained use of effective contraception. By the end of six months, this arm almost eliminated the occurrence of unplanned pregnancies. The intervention also shifted beliefs: women who attended the infertility session were less likely to agree that contraceptives damage fertility, and the change in beliefs closely matched the change in behaviour. An instrumental variables estimate suggests that eliminating infertility fears would more than triple contraceptive use in this population.
Figure 2: Contraceptive use over time, by treatment arm
Policy implications: Family planning in sub-Saharan Africa
Our findings suggest that incorrect beliefs and medical distrust are first-order barriers to using contraceptives to delay first-births among young Zambian women. Reducing cost and travel barriers brought students to clinics, but these changes alone did not generate lasting adoption. Sustained use required addressing fears about infertility directly.
Family planning policies in sub-Saharan Africa have typically focused on married women who already have children, often with the goal of reducing or spacing births. Yet the timing of entry into motherhood is equally important. For young women in higher education, an early first birth can cut short schooling and reshape life chances. Addressing the fears that prevent contraceptive use at this stage is critical if family planning is to deliver the same transformative benefits it once did in the US and Latin America.
Our experiment shows that beliefs about contraception can be changed, and that when they change, behaviour follows. Fear of infertility is widespread, powerful, and central to understanding low contraceptive use among young African women. Yet it is not immutable. Clear explanations, credible messengers, and personal stories reduced misinformation, raised contraceptive use, and lowered pregnancies within just six months.
The contraceptive revolution that transformed opportunities for women elsewhere may still come to sub-Saharan Africa, but access alone appears to be insufficient. Addressing incorrect beliefs may be critical if young women are to gain the power to delay motherhood and realise the full returns to their education.
References
Ahinkorah, B O, E Budu, R G Aboagye, E Agbaglo, F Arthur-Holmes, C Adu, A G Archer, Y B G Aderoju, and A-A Seidu (2021), “Factors associated with modern contraceptive use among women with no fertility intention in sub-Saharan Africa: Evidence from cross-sectional surveys of 29 countries,” Contraception and Reproductive Medicine 6(1): 22.
Bailey, M J (2006), “More power to the pill: The impact of contraceptive freedom on women’s life cycle labor supply,” Quarterly Journal of Economics 121(1): 289–320.
Bau, N, D J Henning, C Low, and B Steinberg (2024), “Family planning, now and later: Infertility fears and contraceptive take-up,” NBER Working Paper.
Boivin, J, J Carrier, J M Zulu, and D Edwards (2020), “A rapid scoping review of fear of infertility in Africa,” Reproductive Health 17(1): 142.
Engelbert Bain, L, H Amu, and E E Tarkang (2021), “Barriers and motivators of contraceptive use among young people in sub-Saharan Africa: A systematic review of qualitative studies,” PLoS One 16(6): e0252745
Goldin, C and L F Katz (2002), “The power of the pill: Oral contraceptives and women’s career and marriage decisions,” Journal of Political Economy 110(4): 730–770
Graeber, T, C Roth, and F Zimmermann (2024), “Stories, statistics, and memory,” Quarterly Journal of Economics, qjae020
Malmendier, U and L Veldkamp (2022), "Information resonance", University of California, Berkeley.