



Mortality among infants significant increased during the first nationwide COVID-19 lockdown in India, not because infants were infected, but because the pandemic disrupted healthcare access, worsened economic conditions, and discouraged mothers from seeking hospital care. Using nationally representative data, we provide the first systematic evidence of this hidden but significant indirect toll on infants in India.
India was among the countries most severely affected by the COVID-19 pandemic, with more than three million deaths and tens of millions of infections (Jha et al. 2022, WHO 2024). When the Indian government imposed a strict nationwide lockdown in April 2020, unemployment rates skyrocketed from 8% to over 20%, and average incomes fell by nearly 44% (Bertrand et al. 2021). Hospitals became overwhelmed with COVID-19 patients, transportation came to a standstill, and millions of people avoided healthcare facilities out of fear of infection. The Oxford COVID-19 Government Response Tracker recorded India’s stringency index as 98.64 out of 100 in April 2020 – among the highest in the world – capturing the severity of restrictions on movement, workplaces, and public gatherings.
These disruptions particularly affected vulnerable populations such as pregnant women and infants, as early-life survival depends critically on timely access to maternal care, safe delivery, and essential health services. Even short interruptions to these services can have immediate and severe consequences for infant health. We present the first survey-based evidence on infant mortality in a developing country during the COVID-19 pandemic.
Comparing infants born before and during the lockdown
We use nationally representative data from the National Family Health Survey on 17 states and union territories representing about 51% of India's total population (Asker, Dhongde, and Shonchoy 2025). The Indian government ordered a nation-wide lockdown in April 2020, which continued until the end of May 2020 and then was partially relaxed between June and September 2020 in districts with a low number of COVID-19 cases (IMF 2023).[1] We focus on the period between April and September 2020, when the nationwide lockdown and mobility restrictions were most severe.
We use an event-study design and a difference-in-differences approach to compare mortality rates of infants less than six months old between two birth cohorts: infants born between October 2018 and September 2019 and infants born between October 2019 and September 2020, where the latter cohort experienced the pandemic and lockdown between April 2020 and September 2020. By comparing infants across these two groups over the same calendar months, we isolate how mortality changed during the pandemic period while accounting for seasonal variation, regional differences, and household characteristics.
Figure 1 shows how infant mortality changed around the COVID-19 lockdown for cohorts born before and during the pandemic. There are no clear differences before April 2020. However, once the nationwide lockdown begins, infant mortality for babies born during the pandemic increased sharply compared to those born earlier and remained elevated throughout the lockdown period.
Figure 1: Changes in infant mortality around the COVID-19 lockdown
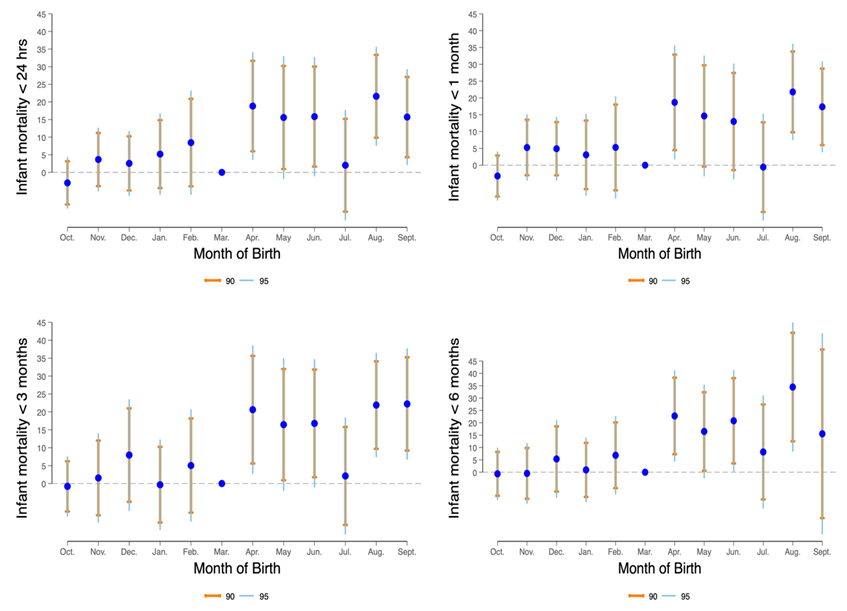
Notes: This figure shows how infant mortality at different ages changed around the COVID-19 lockdown, comparing births before and during the pandemic. Estimates are shown for the six months before and after April 2020, with March 2020 as the baseline. Dots show the estimated effects and error bars show 90% and 95% confidence intervals.
The impact on mortality among infants
Figure 2 summarises the magnitude of these effects across different infant age groups. Mortality increased by approximately nine additional deaths per 1,000 live births within the first month of life, 13 additional deaths per 1,000 live births within three months, and 16 additional deaths per 1,000 live births within six months, compared to the pre-pandemic cohort. These estimates correspond to increases of 30%, 42%, and 44%, respectively. As these measures are cumulative, the estimates rise with age, reflecting the accumulation of health risk over time.
To put these numbers in perspective, the neonatal mortality rate during this period was pushed back by more than a decade, to levels last seen in India in 2004. These findings are consistent with UNICEF projections of a 36.5% increase in neonatal mortality in India between April and June 2020, and with broader estimates suggesting that income shocks from the pandemic led to nearly 100,000 excess infant deaths in India alone in 2020 (Shapira et al. 2021).
Figure 2: Increase in infant mortality during the COVID-19 lockdown
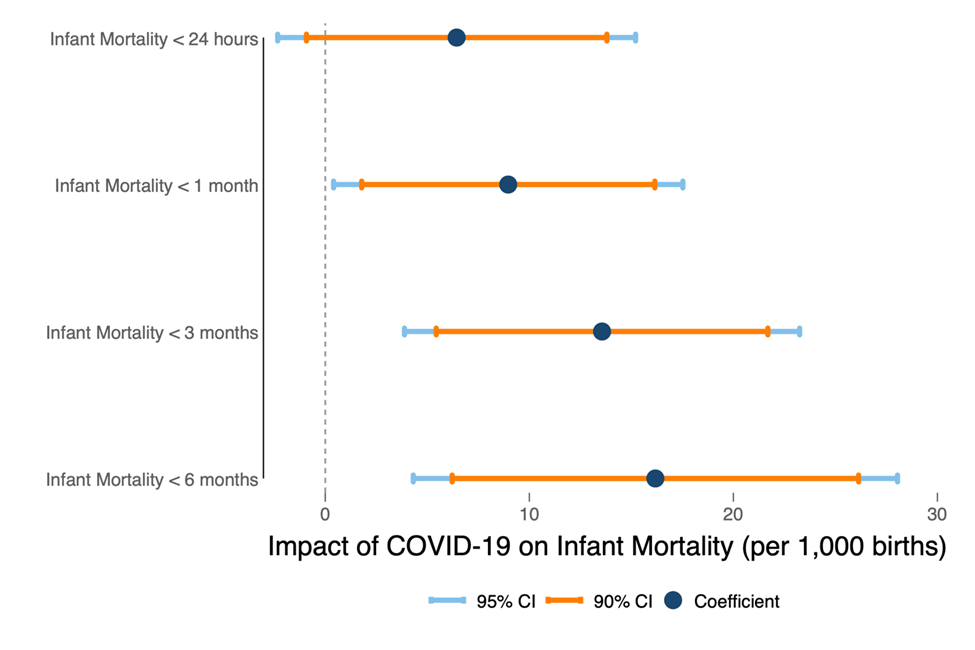
Notes: This figure shows estimated differences in outcomes between infants born before and during the COVID-19 period, comparing cohorts born between October 2018–September 2019 and October 2019–September 2020. Dots show estimated effects, and bars indicate uncertainty (95% confidence intervals).
Indirect effects of the pandemic on mortality among infants
The rise in infant mortality appears to be driven primarily by indirect effects of the pandemic rather than the direct health impact of COVID-19 on infants. COVID-19 had a limited direct impact on infant mortality (Goldstein and Lee 2020, UNICEF 2022). But the pandemic and resulting lockdown led to income shocks to households, reduced healthcare access, increased stress among pregnant mothers, and reduced healthcare-seeking behaviour due to fear of infection.
Several mechanisms are consistent with this pattern. First, access to maternal healthcare declined. We observe reductions in institutional deliveries and overall maternal healthcare utilisation during the lockdown. Mothers were 1.5 percentage points less likely to give birth in a hospital or healthcare facility, and the maternal healthcare utilisation index – covering antenatal visits, nutritional supplementation, and clinical monitoring – fell by about 3% of a standard deviation (Asker et al. 2025).
Second, vaccination coverage declined sharply. Infants born during the lockdown were significantly less likely to receive essential birth-dose vaccines on time. On-time BCG vaccination fell by 6 percentage points, polio vaccination by 4 percentage points, and hepatitis B vaccination by 5 percentage points. Previous research shows that timely vaccination plays a key role in reducing infant mortality (Aaby et al. 2005, Roth et al. 2006). Researchers have documented disruptions to vaccination programmes globally during the pandemic (UNICEF 2021), and our findings suggest that these disruptions had immediate consequences for infant health in India.
Third, behavioural responses played a key role. There is evidence that individuals avoided healthcare facilities due to fear of infection, particularly for maternal and prenatal care (Bisht et al. 2021). This avoidance likely reduced access to timely care at critical stages in pregnancy and the newborn period. Finally, worsening economic conditions – rising unemployment and falling household incomes (Bertrand et al. 2021) – further constrained access to nutrition, healthcare, and other essentials for infant survival.
Policy implications: Maternal and infant health during public health crises
The Indian government took measures early in the pandemic by adding pregnant women to the high-risk group and providing guidelines for maternal health services and prenatal care (Chawla et al. 2020, Singh et al. 2021b). Despite these measures, we believe that there were indirect effects of the pandemic described above which resulted in a rise in infant mortality in the country.
Our findings highlight the importance of maintaining access to essential healthcare services during public health crises. Maternal and neonatal care – including antenatal services, safe institutional deliveries, and postnatal care – should remain accessible even during lockdowns. Governments must prioritise vaccination programmes and adapt delivery through mobile outreach and community-based services. Policymakers also need to address behavioural barriers to care by promoting clear communication and building trust in healthcare systems.
References
Aaby, P, K Hedegaard, M Sodemann, E Nhante, J E Veirum, M Jakobsen, I Lisse, H Jensen, and A Sandstrom (2005), "Childhood mortality after oral polio immunisation campaign in Guinea-Bissau," Vaccine, 23(14): 1746–1751.
Asker, E, S Dhongde, and A S Shonchoy (2025), "COVID-19 and mortality among infants: Evidence from India," Journal of Health Economics, 101: 102991.
Bertrand, M, K Krishnan, and H Schofield (2021), "How are Indian households coping under the COVID-19 lockdown? Eight key findings," Unpublished manuscript.
Bisht, R, R Saharia, and J Sarma (2021), "COVID-19 and the burden of ill-health: A double crisis of disruptions and inequalities," Journal of Social and Economic Development, 23: 342–356.
Chawla, D, D Chirla, S Dalwai, A K Deorari, A Ganatra, A Gandhi, N S Kabra, P Kumar, P Mittal, B J Parekh, et al. (2020), "Perinatal-neonatal management of COVID-19 infection — guidelines of the Federation of Obstetric and Gynaecological Societies of India (FOGSI), National Neonatology Forum of India (NNF), and Indian Academy of Pediatrics (IAP)," Indian Pediatrics, 57: 536–548.
Goldstein, J R, and R D Lee (2020), "Demographic perspectives on the mortality of COVID-19 and other epidemics," Proceedings of the National Academy of Sciences, 117(36): 22035–22041.
Jha, P, Y Deshmukh, C Tumbe, W Suraweera, A Bhowmick, S Sharma, P Novosad, S H Fu, L Newcombe, H Gelband, et al. (2022), "COVID mortality in India: National survey data and health facility deaths," Science, 375(6581): 667–671.
Roth, A, M Garly, H Jensen, J Nielsen, and P Aaby (2006), "Bacillus Calmette-Guérin vaccination and infant mortality," Expert Review of Vaccines, 5(2): 277–293.
Shapira, G, D de Walque, and J Friedman (2021), "How many infants may have died in low-income and middle-income countries in 2020 due to the economic contraction accompanying the COVID-19 pandemic? Mortality projections based on forecasted declines in economic growth," BMJ Open, 11(8): e050551.
Singh, K, D Kondal, S Mohan, S Jaganathan, M Deepa, N S Venkateshmurthy, P Jarhyan, R M Anjana, K V Narayan, V Mohan, et al. (2021), "Health, psychosocial, and economic impacts of the COVID-19 pandemic on people with chronic conditions in India: A mixed methods study," BMC Public Health, 21: 1–15.