



Female politicians in India expand reproductive healthcare, but spousal conflict over number of sons can turn contraceptive gains into domestic violence.
In September 2023, India passed the landmark Women's Reservation Bill, which will reserve one-third of seats in national and state parliaments for women. A large body of research shows that female politicians deliver better outcomes for women – from reduced maternal mortality (Bhalotra et al. 2023) to improved girls' education (Beaman et al. 2012) to more gender-sensitive public goods (Chattopadhyay and Duflo 2004). While this evidence suggests that the Bill should unambiguously benefit women, our research shows that the implications may be more complicated.
Examining state-level elections across India, we find that female politicians significantly improve access to reproductive healthcare for rural women, leading to greater use of modern contraception and better birth spacing. However, these gains come with an unintended cost: in households where husbands want more sons, wives' greater contraceptive use triggers marital conflict and increases intimate partner violence against women (Anukriti, Erten, and Mukherjee forthcoming).
The impact of female leaders
Our work focuses on state legislative assembly (MLA) elections in India. Unlike village council seats, which are subject to gender-based reservation quotas, state assembly seats carried no such quotas until September 2023. This means that female MLAs are genuinely elected on the basis of competition; they wield real decision-making power over local budgets, implementing welfare schemes and influencing the delivery of local public goods and healthcare services.
To identify the causal effect, we use a well-established research strategy based on closely contested elections between male and female candidates (Bhalotra and Clots-Figueras 2014). When an election is decided by a very narrow margin, the gender of the winner is effectively determined by chance. By comparing outcomes in constituencies where women narrowly win against those where men narrowly win, we can isolate the impact of having female leaders.
We combine data from India's National Family Health Survey (NFHS 2015-16) with the District-Level Household and Facility Survey (DLHS 2012-14) and constituency-level electoral data from the Election Commission of India for our analysis.
Female leaders invest in women's reproductive healthcare
Our first key finding is that districts with more female MLAs have better rural public health infrastructure (Figure 1). Electing one additional female politician in a district increases access to community health centres, government hospitals, and primary health centres. Given that 77% of contraceptive users in our rural NFHS sample report that the most recent source for their contraceptive method was a public provider, we expect this improved access to public health facilities to also translate into better access to family planning. Female leaders also improve the availability of female healthcare workers – Auxiliary Nurse Midwives (ANMs) and female doctors – who are on the frontlines of delivering family planning services in rural India. Women's community groups (mahila mandals) also become more prevalent. Beyond infrastructure, female MLAs also accelerate the implementation of flagship government programmes targeting women's and girls' health.
These results are consistent with research showing that female leaders tend to prioritise policies that directly benefit women (Chattopadhyay and Duflo 2004, Clots-Figueras 2011), and that they are particularly effective at mobilising female grassroots health workers (Goyal 2023).
Figure 1: Improvements in rural health infrastructure and programme implementation
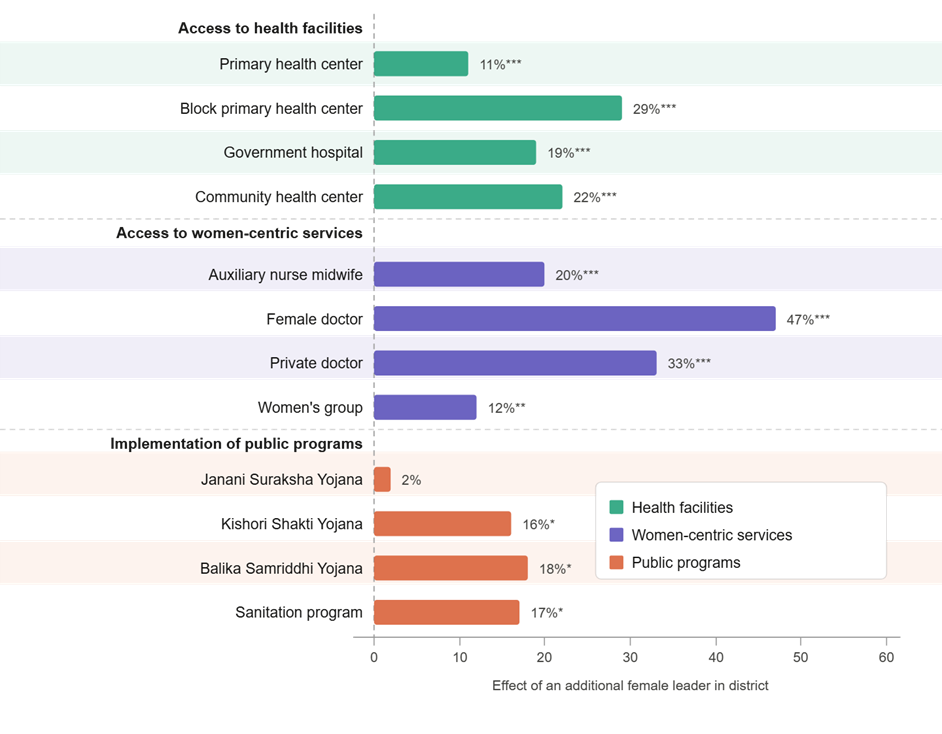
Notes: This figure presents the percentage improvements in rural health infrastructure and implementation of public programs due to the election of an additional female politician in a district based on the 2SLS estimates presented in Anukriti et al. (forthcoming). Stars denote statistical significance of the findings.
Greater access increases contraceptive use and birth spacing
Does greater public provision of reproductive healthcare services translate into real changes in women's reproductive choices? Yes, meaningfully so. We find that electing one additional female politician in a district increases modern contraceptive use among rural women by 8–10% and the number of years between births by roughly a quarter of a year on average. These are important gains: short intervals between pregnancies are associated with higher maternal mortality and complications, and greater control over fertility can improve women's education and labour market participation (Miller and Babiarz 2016, Canning and Schultz 2012).
The unintended consequence: A rise in intimate partner violence
Alongside these positive findings, we find a troubling unintended consequence. Exposure to female leaders increases the likelihood that rural women report experiencing physical violence from their husbands (Figure 2).
This effect is concentrated among younger women still in their childbearing years, and especially among women whose husbands desire more sons than the couple currently have. In India, son preference remains widespread (Jayachandran 2023): in our sample, 30% of husbands express a desire to have more sons than they currently have, and 44% of couples disagree on their ideal number of sons. When wives gain better access to contraception through improved healthcare, some husbands, particularly those with strong son preference, appear to respond with violence.
Figure 2: Change in physical IPV experienced by female constituents
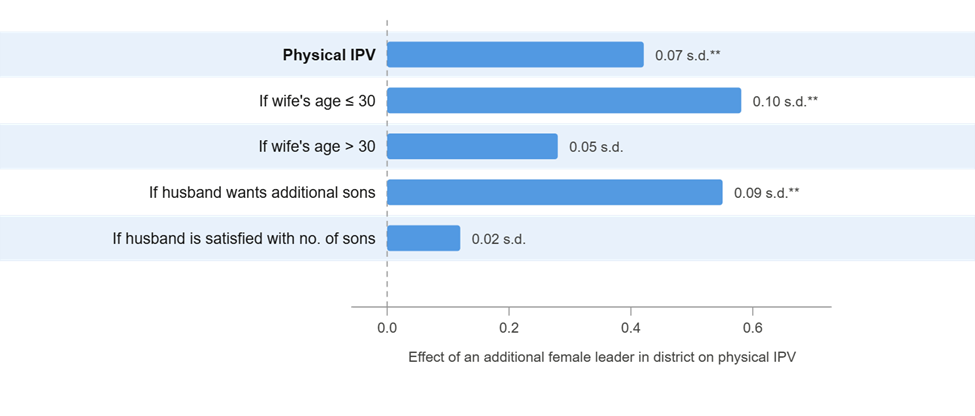
Notes: This figure presents the change in physical IPV experienced by female constituents (in standard deviations (s.d.)) due to the election of an additional female politician in a district based on the 2SLS estimates presented in Anukriti et al. (forthcoming). Stars denote statistical significance of the findings.
This mechanism is consistent with evidence from a randomised experiment in Zambia (Ashraf et al. 2014), which found that when women received access to family planning services without their husbands' knowledge, they were more likely to use concealable contraception but also experienced greater marital conflict. Similarly, research in India has shown that female sterilisation can increase spousal violence (Anukriti 2020). The common thread is spousal disagreement over fertility decisions, and the violence that can result when women exercise reproductive autonomy in the face of that disagreement.
We rule out a range of alternative explanations. The rise in IPV is not explained by changes in attitudes toward violence, shifts in women's employment, or changes in who women marry. Nor is it driven by increased reporting of violence. The evidence points clearly to the contraceptive use: son preference conflict as the key mechanism.
Policy implications
These findings carry important lessons as India implements the Women’s Reservation Bill. The policy takeaway is not that there should be fewer female leaders – far from it. Our evidence shows that female politicians are, on average, genuinely good for women: they strengthen health infrastructure, expand access to family planning, and increase women’s ability to control the timing of births. These are meaningful gains that are likely to improve women’s wellbeing in important ways.
At the same time, our results show that empowerment reforms can have unintended harmful effects when they collide with deeply entrenched gender norms and disagreements within households over fertility, especially when husbands have stronger son preference (Borker et al. 2026). In that setting, greater access to contraception and reproductive healthcare can improve women’s choices while also increasing the risk of violence at home. The lesson, therefore, is not to slow progress on women’s political representation, but to pair it with complementary policies that protect women and address the conditions that generate backlash.
One concrete response may be to equip healthcare professionals with training to recognise victims of intimate partner violence and connect them to local support, such as shelters, hotlines, counselling services, legal assistance, and other tailored resources. As female leaders expand health access, those encounters with the health system can become critical entry points for identifying abuse and helping women reach support.
More broadly, stronger coordination between healthcare providers and law enforcement could help women better understand their legal rights and seek redress. Complementary efforts to address spousal misalignment in fertility decision-making may also be essential. The Women’s Reservation Bill remains a historic and important reform. But for its benefits to reach women fully and safely, representation reforms should be accompanied by a wider strategy that tackles the household dynamics this research brings to light.
References
Anukriti, S (2020), "Female sterilization and women's well-being in India," Unpublished manuscript.
Anukriti, S, B Erten, and P Mukherjee (forthcoming), "Female leaders and intrahousehold dynamics: Evidence from state elections in India," American Economic Journal: Economic Policy.
Ashraf, N, E Field, and J Lee (2014), "Household bargaining and excess fertility: an experimental study in Zambia," American Economic Review, 104(7): 2210–37.
Beaman, L, E Duflo, R Pande, and P Topalova (2012), "Female leadership raises aspirations and educational attainment for girls: A policy experiment in India," Science, 335(6068): 582–586.
Bhalotra, S, and I Clots-Figueras (2014), "Health and the political agency of women," American Economic Journal: Economic Policy, 6(2): 164–97.
Bhalotra, S, D Clarke, J F Gomes, and A Venkataramani (2023), "Maternal mortality and women's political power," Journal of the European Economic Association, 21(5): 2172–2208.
Borker, G, J Eeckhout, N Luke, S Minz, K Munshi, and S Swaminathan (2026), "Wealth, marriage, and sex selection," American Economic Journal: Applied Economics, 18(2): 107–146.
Canning, D, and T P Schultz (2012), "The economic consequences of reproductive health and family planning," Lancet, 380(9837): 165–171.
Chattopadhyay, R, and E Duflo (2004), "Women as policymakers: Evidence from a randomized policy experiment in India," Econometrica, 72(5): 1409–1443.
Clots-Figueras, I (2011), "Women in politics: Evidence from the Indian states," Journal of Public Economics, 95(7–8): 664–690.
Goyal, T (2023), "Representation from below: How women's grassroots party activism promotes equal political participation," American Political Science Review, 118(3): 1–16.
Jayachandran, S (2023), "Ten facts about son preference in India," Unpublished manuscript.
Miller, G, and K S Babiarz (2016), "Family planning program effects: Evidence from microdata," Population and Development Review, 42(1): 7–26.